




Introduction – disability and impairment
In 2021 some 24 volunteers from The Western Front Association transcribed the key details from 25,000 pension ledger records for soldiers, naval and air force personnel.
The pension ledgers use the word ‘disability’. Modern disability studies and the associated social model of disability make a distinction between impairment and disability. ‘Impairment is based purely on physical difference, while disability is a social issue: the former does not simply “cause” the latter, social barriers do, such as restricted access to medical activities, educational institutions and welfare provision. A medical model which sees disability solely as an individual, personal tragedy in need of cure has been categorically rejected’.[1]
War, health & longevity
The negative effect of the war on general health is a given. Noonan has estimated that three per cent of Australian veterans who saw active service in the Great War, and who survived the conflict, would die a premature death due to war-related causes in the post-war years.[2] In a war where at least 40% of those who served became casualties and 27% received pensions, this is sadly not surprising.
A study of soldiers leaving New Zealand in 1914 to fight and who survived, shows that in comparison to a non-combat 1918 cohort, veterans lived for 1.7 years less.[3] This difference is perhaps not that great given the circumstances, yet significant to the individuals concerned and their loved ones in an era where lives were shorter than in our modern world. The effects of wounds, illness and suicide all played a part in this difference, and the effect did not last beyond 1930. This is interesting, as it suggests that there was a limited period in which the war’s physical and psychological effects played their part in life-expectancy.
The wider community of impairment
The war of course left many individuals physically impaired through wounding. As Joanna Bourke summarises, for instance, over 41,000 men had limbs amputated during the war and 272,000 suffered limb injuries that did not require amputation.[4] Yet, as Bourke reflects, those affected joined a wider community of impaired men, women and children. Thus, in 1919, there were 8.6 ‘crippled’ children per every 1,000 in Britain.[5] During the 1920s there were over 200,000 industrial injuries of varying severity a year, 40,000 in the coal industry alone.[6]
On one hand, therefore, the impaired of the Great War were a very significant group; on the other, they need to be placed in the wider context of the prevalence of impairment in post-war society.
Impairment and the environment
In terms of the broader notion of disability, the homes that impaired soldiers returned to may not have been ideal environments – a damp, poorly heated house may have been an unhelpful situation for men with lung conditions, for instance. The poverty-related matters that continued to affect the population’s health in the pre-war years may have impacted disproportionately on the war-impaired.
At home, individuals may have had to lie on a sofa or bed, or propped up in an armchair ‘in the one living room of the household, where ordinary domestic routines continued’.[7] In respect of the latter, a wife as potential caregiver may have had further daily burdens placed on her, and the marital relationship may likely have suffered. The impact may have extended to children, either forced into work earlier, or denied this opportunity by having more household care tasks imposed on them.
An impaired or convalescing soldier may have been removed from ‘his “masculine” public sphere of work and, possibly, from community social life and confined him to the “feminine” private sphere of home’.[8] Such individuals would have been familiar sights in the street, yet some may have been unable to make the physical journey to their working men’s club or church, and such popular physical activities like football may well have been denied them.
Such experiences should not be drawn in simplistic lines however – men adjusted, taking up other activities of a less ‘masculine’ nature, and enjoyed them. Ex-servicemen may have had fewer social activities, but those they did partake in may have had higher valency, e.g. engaging with ex-comrades.
This is the trues cope of ‘disability’, and it is complex, ‘dependent on so many different factors and intersections, and dependent on personal dynamics’.[9]
The Ministry of Pensions
In wider British society, the acceptance of the need for statutory systems of welfare had begun with the Employer’s Liability Act of 1870, and continued with the Workmen’s Compensation Act of 1880 and its subsequent revisions. Within the military, however, a system of daily allowances been introduced in 1685 for disabled non-commissioned officers and other ranks, administered by the Royal Hospital, Chelsea. This was codified further in the (military) Pensions Act of 1806. The conditions of service for men who volunteered for the Imperial Yeomanry in the Second Boer War (1899-1902) included ‘pensions and gratuities to be paid according to Regular Army rates’, and the first state pensions for the widows of rank and file soldiers were introduced in 1901.

Above: Ministry of Pensions, Acton
Establishing the Ministry
‘At the beginning of 1916, there were four key departments dealing with pension administration, these were The War Office, The Chelsea Commissioners, The Army Pensions Issue Department and the Statutory Committee for supplementary pensions. In addition, the Local Pension Committee assisted men in dealing with queries and submitting pension claims for missed claims or changes in circumstances. In November 1916 the majority of this work, with the exception of Army Service Pensions, Naval Pensions and Separation Allowances, was proposed for merger under a single controlling board which would oversee the work of the hundreds of Local Pension Committees.
Thus, in February 1917 the Minister of Pensions took control of all disability, widows and dependent pensions’.[10]
The 1919 War Pensions Act made the right to a pension statutory and introduced a right of appeal, the 1921 WPA introducing a Final Awards Scheme and a seven-year time limit on claims.
The structure and tasks of the Ministry
Outside of providing medical and surgical treatment, managing of Ministry hospitals etc., providing medical supplies and equipment, and providing training for the impaired within special institutions, the Ministry of Pensions had to set up medical assessment boards. In organising this it decentralised in 1919 and set up 11 regional offices, and in terms of the surviving records, Scotland, Northern Ireland, Southern Ireland, North-West England, Northern England, East Midlands, West Midlands, South-West England, and Wales were used in this study.[11] The use of regions was a temporary expedient, and once of the crest of the wave of assessments passed, the Ministry assimilated the regions.
Assessing impairment
The assessors partly comprised full-time medical officers, partly sessional doctors, with additional the use of doctors in private practice, specialists and others on a per report basis. Each board was originally composed of three doctors, and there were ‘Primary Awards’ boards, ‘Re-Survey’ boards (assessing those whose pensions were due to expire, and those who claimed their conditions had worsened), and ‘Appeal’ boards where a specialist in the particular impairment was drafted as one of the members. (This may well be the cause of the observed occurrences of grouping of records together in relation to similar conditions). Doctors were often ex-servicemen themselves. 1,051,102 boards were held 1919-20, dropping to 47,424 1928-29.
The doctors had firstly to assess whether the impairment was consequent upon war service, or aggravated thereby. The degree of impairment then had to be assessed. As the Official History (Statistics) notes, ‘a problem of this kind was new to the majority of the profession’. This came to be a matter of dispute for the assessing doctors. ‘The Ministry … took as its standard the normal healthy man of the same age as the pensioner and assess the degree of disablement arising from the wound or disease according to the extent to which war service had reduced in below that standard.’[12] It may be surmised that a ‘normal healthy man’ in this era was difficult to define.

Above: Categories of degree of impairment (Ministry of Pensions leaflet c. 1920).
Assessing doctors were required to rate men as per cent disabled from 100% dropping by 10% stages until 20% was reached, when they could then use the notion of ‘less than 20%’. Many used the bands of, for example, 14-19%, or small percentages of 5% or even 1%. A Ministry of Pensions leaflet dated c.1920 sets out the tariff of proportion (above) of pension corresponding to degree of disablement in relation to various conditions. 100% disability accrued a weekly pension of 40/-, with additions for wife and children. A period for which the pension was payable was specified, but sometime ‘for life’.
The average weekly wage in 1920 was:[13]
Bricklayer 97/-
Labourer (building) 84/-
Fitter 89/-
Engine driver 84/- to 102/-
Goods porter 62/- to 68/-
Agricultural labourer 42/- to 46/-
The pension ledgers
The ledgers (commenced when the regional system was set up) comprise 15,000 ‘books’, covering 1.5 million pages. Somewhere approaching 1.2 million records exist concerning other ranks who survived the war (officers do not feature in the pension ledgers). Given that 1.6 million service personnel were awarded pensions, the extant ledgers do not cover the entirety of the affected population.
Above: A 'typical' pension ledger, showing the dimensions
The issues described above concerning assessing impairment are borne out in inspection of the pension ledger records, which comprise two pages. The legend relating to attributability reads: ‘State whether attributable to or aggravated by service or non-attributable’.
Sometimes a percentage appears following ‘aggravated’ or ‘attributable’ on the first page. This is likely a duplication of the percentage disability recorded on second. However, given that these percentage ratings varied, this figure sometimes matches only one rating on the rear (second page), but occasionally none of them. Such recordings of a percentage against attributability on the front pages are in the minority. The clumping together of records marked in this way suggests either the work of a particular clerk, or even particular doctors/boards (when similar conditions clump together in a series of first pages).
The first and second pages thus represent the extent of disability and attributability to service. It is also notable that a condition could be ‘attributable’, yet there might be ‘nil’ disability. (It should also be noted, where original pension files exist, a higher disability rating may be given as the first rating). For the purposes of this research, the final disability rating is used, as likely to reflect the continuing effect on the serviceman’s life.
Examples of the first and second pages of a pension ledger appear on the following page, being the pension ledger record of Lance-Sergeant (290466) Thomas Chance, Monmouthshire Regiment (b. 1886 and married). He lived in Tredegar, Monmouthshire, but had been born in Lye, Worcestershire, and in 1911 worked as a ‘coal miner (hewer)’.
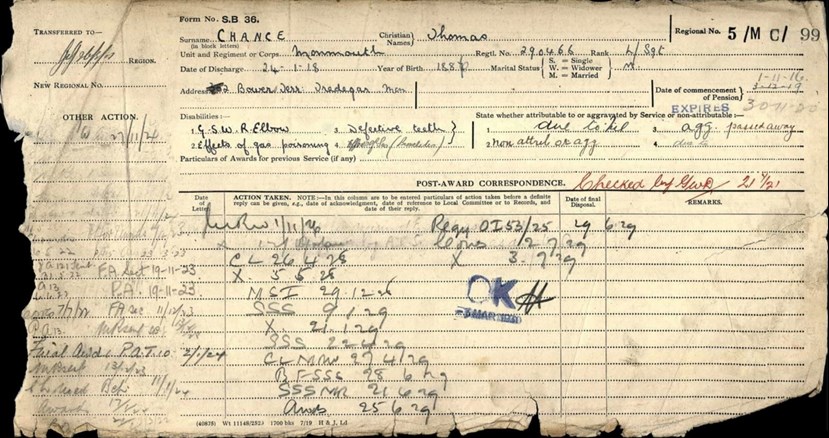
Above: Front of ledger record.


Above: The listed conditions are gunshot wound (GSW) right elbow (due to, but indicated as ‘nil’ disability); effects of gas poisoning (bronchitis) (due to) and defective teeth (aggravated). His pension commenced on 1 November 1916 (he was discharged on 24 January 1918) expiring 30 November 1918, clearly re-boarded with references continuing to 1929. ‘Passed away’ is noted. He was miner prior to the war, and went to the Western Front in February 1915.
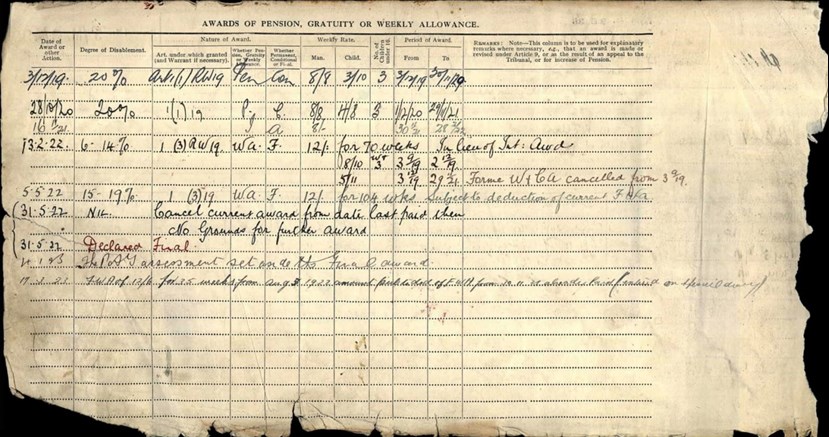
Above: Rear of ledger record. Between 03/12/1919 and 05/05/1922 he was rated 20% to 15-19% disabled. On 31//05/1922 he was declared to have ‘nil’ disablement, and his award was declared ‘final’, with ‘no grounds for further award’.
Generosity of dealing with servicemen and malingering
It may be speculated (judging from runs of similar ratings of ‘attributable’ or ‘aggravated’ in the ledgers) that there were two types of medical assessors, ones who were more ‘generous’ (many had, of course, been on military service themselves), and those who were less generous.
Captain Lawrence Gameson, a medical officer, was clearly one of the former. He expressed ‘the greatest contempt’ for the Ministry, writing that it was ‘under no obligation automatically to regard almost every claim as suspect; which it did, summoning medical and surgical yes men to help it wriggle out of its minimal responsibilities’.[14]
In overall consideration of these assessments, no doubt there is some balancing between servicemen overstating the degree of their medical problems and this less generous approach.
To what extent was malingering a factor in pension claims? Malingering was certainly an issue during the war itself. Bourke describes three categories of malingering,[15] ‘actions aimed at avoiding the armed forces altogether, those aimed at prolonging incapacity and those aimed at being sent back from active service. She describes various sources which indicate how men ‘imbibed drugs such as digitalis, belladonna and thyroid extract to produce circulatory disturbances. They pricked their tonsils in order to cough up blood. Albuminaria was feigned by the addition of egg-albumen to urine. Inhaling pipe smoke before the examination might result in palpitations of the heart’. An inflammation of the knee could be produced by needle coated in caustic black powder pushed into the joint cavity, whilst ‘Soldiers hawked specimens of saliva containing tuberculosis bacilli to their mates’.
These examples are, of course, recorded during the war itself. To what extent they occurred during the pension examination process is unknown. In terms of the wider work environment, Sir John Collie estimated in 1916, studying 3,667 industrial accidents, that 8% of cases were feigned,[16] but the following year ratcheted up his estimates, concluding that ‘one in every four injured workmen was fit for work’.[17] Doctors were certainly trained to spot malingering. Conditions are crossed out in the pension ledgers, but this is more likely to be in indication that such had resolved.
In terms of the nation’s generosity, the Government (perhaps naturally) became alarmed at the extent of the pensions bill, especially as veterans aged. ‘The annual war pension budget was £106,600,000 – around seven per cent of national government expenditure. A Committee on National Expenditure facilitated a drive for retrenchment in public spending in the early 1920s. It enforced a host of subsequent reductions in social spending in education, health, housing, welfare, and unemployment benefits. The Ministry restricted its future liability in its resulting 1921 War Pensions Act by introducing a seven-year time limit on claims from a veteran's military discharge or from 1 September 1921 depending on which occurred first. The Ministry's seven-year time limit was successful in its prevention of further liability and so reducing costs.
Between 1921 and 1939, Ministry annual spending decreased by over sixty per cent (£106,600,000 to £39,400,000). Lobbying attempts by the British Legion and supportive MPs to introduce bills during successive governments either to relax or remove the Ministry's seven-year time limit were repeatedly rebuffed. Their defeat occurred despite high profile press campaigns with one attempt in 1925 involving an 825,000 strong petition, the largest petition since the Chartists of 1848. The value of pensions, which did not fall in line with the drop in the cost of living as originally planned, by contrast, actually increased during the 1920s. A pensioner on a maximum pension was just three shillings short of a female cotton weaver's weekly wage by 1926, whereas it had equated to just more than half only six years previously. This effectively dampened the Legion's charge that disabled ex-servicemen had been disregarded by the British state helping to rebuff calls for the seven-year time-limit to be altered or removed. However, the Ministry’s simultaneous time limit on claims and maintenance of allowance rates would prove a crucial long-term liability, especially during the Great Depression.’[18]
The WFA pension ledger study
Method
The total number of 25,000 for the pension ledger study (PLS) was arrived at as beyond representative of the whole sample of pension records if statistical techniques were employed in analysis ensuring decreased margin of error and increased confidence level. They can therefore be regarded as representative of the whole 1,600,000. The statistics given in this study are largely descriptive.
The split between Army, Royal Navy, and Air Force in record capture was calculated in terms of the number of servicemen in those arms at the Armistice, 84%, 9% and 7%, respectively.
The data was collected from all areas of the United Kingdom for which ledgers survive (except Yorkshire). In terms of randomisation, individual transcribers were assigned to different regions and set to work on different parts of the ledgers(held on the Fold3 website). In terms of randomisation in other studies, the ‘million card study’ employed two series of hospital admission records, which were investigated in thirds, as the records were organised by regiment. Noonan went to considerable length to achieve randomisation in his study of Australian service records,[19] and would have regarded the British Official History approach as, whilst better than the Australian Official History approach, less stringent than his own.
The details abstracted from the cards included:
Surname/forename
Service/unit
Service no.
Rank
Year of birth
Marital status
Disabilities (1-4)[20]
Attributability
The PIN26 series at the National Archives contains 22,756 pension files, representing 2% (every 50th file) from the London/South-East region. The remaining records from this region were then destroyed. This study therefore covers a slightly larger body of individuals than PIN26, which does not seem to have been subject to an extended prosopographical analysis.
Demographics of the WFA survey population
As per the percentages indicated above, the details of 21,000 Army; 2,250 Navy; and 1,750 Air Force pension applicants was collected.
Whilst there was no reason to divide the RAF claimants in any way as all (perhaps bar one) were ground services, the Navy can be divided into ship crew (including some Marines) and dock workers under one heading; with the Royal Naval Division (RND) as the other.
In the Navy category, 44% of pension claimants were RND, i.e. men who had fought as infantry. To state the obvious, this reflects the fact that that being in the infantry was a more dangerous occupation. It is impossible to be precise about the number of naval personnel who served in the RND – the literature refers to initially 20-30,000 surplus men taken from the Royal Naval Volunteer Reserve. The Royal Naval Division Index lists 50,720 records.
The Army, of course, can be subdivided according to its various branches. The pension ledgers, however, list the final branch that the claimant served in – thus many claimants listed as Labour Corps had been wounded/injured or developed medical conditions as infantry. The category ‘Other’ (see Table 1 below) contained men who had served in branches such as the Tank Corps, Machine Gun Corps, Veterinary Corps, Military Police etc. (A number of pension claimants’ final branch of service in this category was the Royal Defence Corps, which largely contained the particularly unfit and superannuated).
(a) Branch of Army
The percentage of claimants for each branch are set out in Table1, with the relative strengths of those branches at the Armistice.
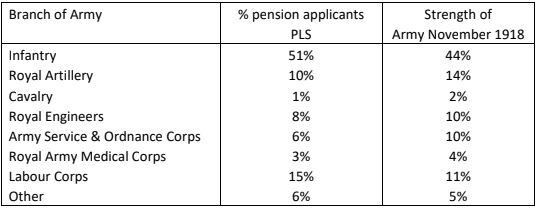
Table 1: Distribution of pension claimants amongst various branches of the Army, compared to their relative strengths at the Armistice.
There is no statistically significant difference between these two sets of figures, and hence the spread of pension applicants is broadly in proportion with the strengths of the various branches of the Army at the Armistice.
(b) Ranks of pensioners
The distribution of ranks is detailed in Table 2:
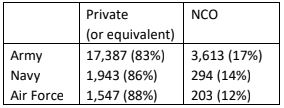
Table 2: Distribution of ranks across services in the PLS
(c) Ages of pensioners
In terms of age, the oldest claimed to have been born in the mid-1850s. Of the youngest, five claimed to have been born in 1903. The average years of birth are shown in Table 3, there being a uniformity across services. The average age on pension assessment in 1919 for the whole cohort was 32-3 years old.
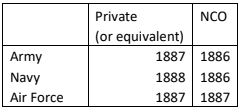
Table 3: Average year of birth by service/rank in the PLS
This analysis is much expanded in Tables 8 and 9 below.
(d) Marital status of pensioners
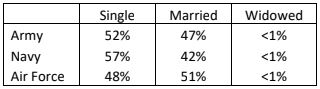
Table 4: Marital status in the PLS
This is only of interest in relation to the fact that a spouse (and dependent children) would be entitled to pension in terms of degree of disablement of the pensioner.
The Official History statistical data
As part of their compilation of the Official History: Medical Services - Casualties and Medical Statistics,[21] [henceforth OH (statistics)], Major T. J. Mitchell and colleagues, considering the ‘11 million odd battle and non-battle casualties’, carried out a detailed analysis of 1,043,653 casualties from the years 1916 to 1920, using the official medical history cards.
Much of the OH (statistics) devotes its consideration to different theatres of war – the purpose, of course, was not simple medical research, rather to prepare the Army’s medical services for future wars in various corners of the Empire.
The figure of 11,000,000 refers to hospital admissions (the figures presented in the OH (statistics) sometimes refer to admissions and sometimes to individuals). A major deficit of the figures presented in the OH (statistics)‘million card’ study is that they do not appear to represent the Air Force and Royal Navy, and if they are present in the pension data, no separation is made. The medical history cards formed the basis of the Ministry of Pensions tabulations, and in the OH analysis were restricted to British servicemen only.
‘11 million odd battle and non-battle casualties’, of course, is a higher figure than those who served. Overall, 2,414,000 individuals, or 40 percent of those who served in the Navy, Army, Air Force or Nursing Services were affected by war service in terms of death or disablement. Service personnel were often wounded more than once, and would also separately become ill. The ’11 million odd’ casualties is therefore an opaque figure.
The ‘million card’ study was based on two sets of sample cards (N=1,043,653) representing 18.5 percent of the cards for the years 1916 to 1920 and were ‘taken as closely as possible in proportion to the approximate strength of the various arms comprising the British Army’.
The OH presents some 30 pages of tables, prefacing them with the remark: ‘They are self- explanatory and require no prefatory remarks’.[22] This is far from the case.
(a) Overall numbers of wound and sickness casualties.
The OH (statistics)‘summary of wounds, diseases and injuries’,[23] giving an apparent ratio of wounds to disease/injury of 1:4 is reproduced as Table 5 below. The table appears to present the two categories as either/or, when, in reality, no such distinction can meaningfully be made.
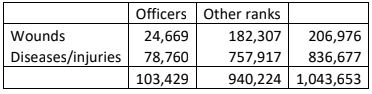
Table 5: Wounds, disease and injury as per the OH
The PLS (Table 6), referring to Army pension claimants alone, for the sake of comparison, reveals the following when the first listed condition only is taken into account:
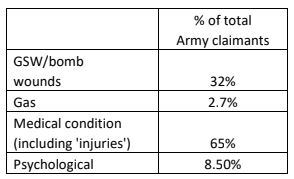
Table 6: Wounds, disease and injury as per the PLS
When individual pension claimants are taken into account, the ratio of GSW to disease/injury in pension claimants is 1:3.
The issue of overlap of conditions
The problem with the OH (statistics) figures (Table 5) presenting disease/injury and wounds as alternatives immediately becomes apparent, as the total of the separately recorded percentages in Table 6 adds up to just over 108%. This brings the issue of overlap of conditions into focus.
Thus, in the PLS:
- 862 claimants (4%) were claiming for both a GSW and a medical condition
- 118 claimants (0.6%) were claiming for both the effects of gas and a medical condition (in the large part unrelated)
- 66 claimants (0.3%) were claiming for both a GSW and the effects of gas, but no separate medical condition
- 593 claimants (3%) were claiming for a psychological condition as well as either a wound or disease
These figures amount to the additional 8 per cent.
It must also be born in mind that the number of GSWs per individual may have been inflicted in one go or on several different occasions, and illnesses were likely sequential. Figures based on hospital admissions are of use to Army planning, but tell us less about the burden of wounding/illness borne by individuals.
(b) Casualty cases by branch of the Army
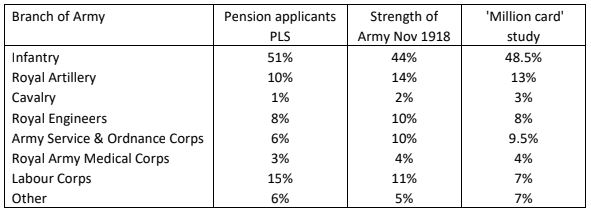
Table 7: Comparison of strengths of each branch of the Army in the PLS and OH studies, compared to that on 11/11/1918
The branches of the Army as described in the ‘million card’ study can be added to the figures of Table 1 (see Table 7). Analysis of variance shows no significant differences even at the p<.10 level. The two studies are thus compatible with the strength of the expanded and developed Army at the end of the war, and pension applicant numbers are proportional to the numbers in particular branches. The one noticeable difference is that the number of Labour Corps pensioners is double in the PLS than in the ‘million card’ study. This reflects the fact that the OH (statistics) uses branch at time of wounding etc. whereas the PLS is based on branch at discharge. It thus demonstrates the shift of unfit men into the Labour Corps (and, when the RAF is considered, into the RAF).
The statistical calculation therefore suggests, importantly, that the PLS results can be viewed as directly comparable with the OH study, and that the number individuals in both is directly reflective of the relative strengths of the Army at the Armistice.
(c) Wounds and disease/injury by age
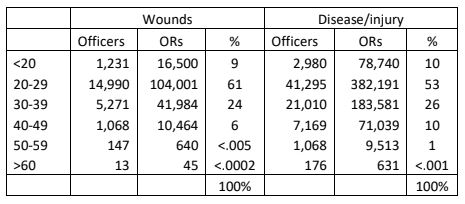
Table 8: Wounds & disease/injury figures as per the OH (statistics)[24]
In respect of Table 8, the OH (statistics) unfortunately does not inform as to whether age is related to date of admission or not, but it may well be assumed that it is. The pension ledgers give year of birth, but not when the wounding/illness occurred –age at the end of the war only can be calculated. The OH (statistics) data of Table 8 does not enlighten us to the interesting matter of what percentage of men of a certain age were susceptible to wounds/disease/injury.
[The OH (statistics)might also give the impression that all diseases noted were attributable to war – the pension ledgers at least inform us whether illness was ‘aggravated’, i.e. a pre-existing condition made worse by war. This is considered later in the section on medical conditions.]
Both the OH and PLS data on age suffer limitations in usefulness of interpretation as we do not know the base rates in terms of ages in the Army. Further, the PLS cannot consider data on officers.
Using the pension ledger data Table 9 calculates what percentage of the pensioner group each age cohort consists of, where it is contrasted with the same re-calculated from the OH (statistics) data. It is also possible to tease out injuries (which the OH data combines in the general medical conditions) and to separate out gas casualties, (which the OH fails to state whether it includes such under ‘wounds’ or not).
Firstly, it can be observed that the two younger age cohorts are represented less in the PLS than in the OH (statistics) hospital admission data. Perhaps the younger group recovered more effectively from whatever ailed them.
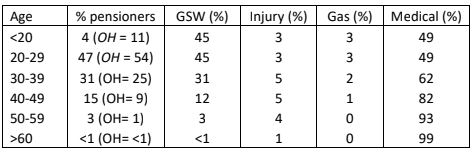
Table 9: Age cohorts in the PLS, based on first reason given for pension claim
Secondly, the likelihood of a gunshot wound being the cause for the pension claim drops from the 40-49 age cohort in terms of a percentage of overall conditions. It is interesting that the number of pension claims for injury holds steady until the over 60 cohort is considered. It is likely that this indicates increasing age rendered individuals less likely to be in teeth arms, yet still vulnerable to injury and illness in other service branches. The percentage of claims primarily for a medical reason accelerates from the 30-39 cohort onwards, indicating age to be a vulnerability in this respect.
The Official History review of Ministry of Pensions data
The OH (statistics) takes the rough calculation that 6,000,000 served (excluding Dominion/Indian troops), and that at the Armistice 600,000 had been discharged as disabled with a pension/gratuity, i.e. 10%.By 31st March 1930, 1,664,000 (or 27.7 %) of those who survived the war (estimated at 5,250,000) had been granted a pension.
Many of these, of course, required hospital care, the organisation of which was one of the Ministry’s tasks. The peak of those receiving institutional treatment was in March 1922 (143,388 – 23,894 as in-patients and 119,494 as out-patients).
The impairments could be broadly classified as:
(i) Immediately obvious and with clearly circumscribed sequelae, such as a clean bullet wound.
(ii) Immediately obvious, but with liability to prolonged and widespread sequelae, such as head wounds and dysentery.
(iii) Not immediately obvious but emerging in due course (the matter of latency), e.g. TB.
Three further classes of impairment were defined:
Class I Obviously stable and permanent
Class II Stabilisation gradually effected
Class III Unstabilised
The proportions of servicemen in these categories is set out below in Table 10.
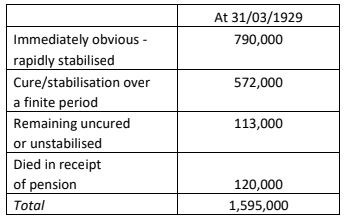
Table 10: Progress of disability resolution as per the OH (statistics)[25]
The broad classification of the bulk of pensionable conditions can be viewed as comprising 12 areas according to the OH (statistics):
(a) Wounds, injuries and amputations
(b) Tuberculosis
(c) Respiratory diseases, excluding TB and gas injury
(d) Organic diseases of the heart
(e) Functional diseases of the heart
(f) Neurasthenia
(g) Malaria
(h) Rheumatism (including fibrositis, myositis, myalgia, pleurodynia, lumbago and sciatica)
(i) Diseases of the ear
(j) Psychoses
(k) Dysentery
(l) Nephritis
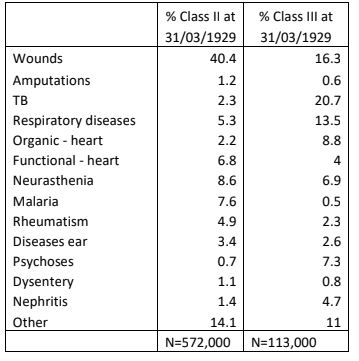
Table 11: Class II & Class III wounds as detailed in the OH (statistics)[26]
As Table 11 shows, wounds, neurasthenia, malaria and functional diseases of the heart constituted the bulk of stabilised Class II as at 31/03/1929; and tuberculosis, wounds, respiratory diseases and organic diseases of the heart formed the major proportion of the unstabilised Class III.
The OH considers ‘First Awards’ (made up to 31/03/1926) as affording ‘a reliable indication of the main characteristics of post-demobilisation awards’. The (amended/recalculated) table of these is presented in Table 12 on the following page.
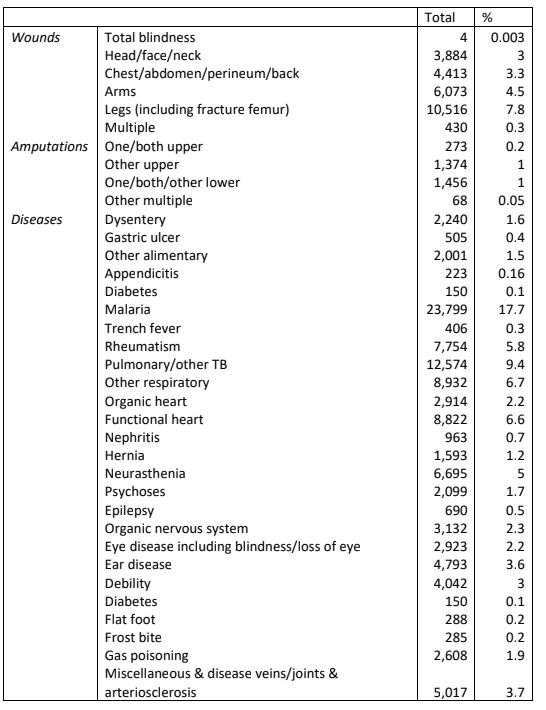
Table 12: Distribution of First Awards as detailed in the OH (statistics)[27]
ANALYSIS OF THE PENSION LEDGER DATA
This is discussed in four sections:
1. Wounding by Enemy Action.
2. Injuries.
3. Medical Conditions.
4. Physiological and Psychiatric Conditions
1. Wounding by enemy action
Seventy-five per cent of the wounds recorded in the OH (statistics) were due to gunshot wounds (GSW - shrapnel & bullet), bomb or bayonet. In the PLS, only nine out of the Army applicants were specifically noted to have suffered bayonet wounds. Twenty-two per cent of wounds were defined as ‘accidental or undefined’ by the OH. The OH also notes that .13 % of GSWs were self-inflicted. In the PLS, only 3 of the 21,000 Army pension applicants were noted to have a self-inflicted wound, the small number being hardly surprising.
(1) Wounds per branch of Army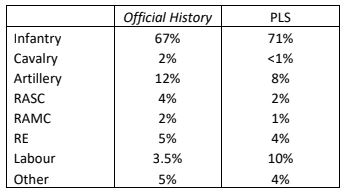
Table 13: Wounds per branch of the Army as per the OH (statistics)[28] and first listed disability as GSW in the PLS
When the fact that the branch of the Army was listed in the pension ledgers as the last recorded at the war’s end is taken into account, the fact that some of those impaired by wounds were transferred into the Labour Corps accounts for the inflated number in the pension ledgers in that category.
Both sets of figures confirm the common sense view that the infantry were far and away the branch of the Army most likely to suffer wounding with the Royal Artillery the next.
(2) Location of wounds in relation to parts of the body
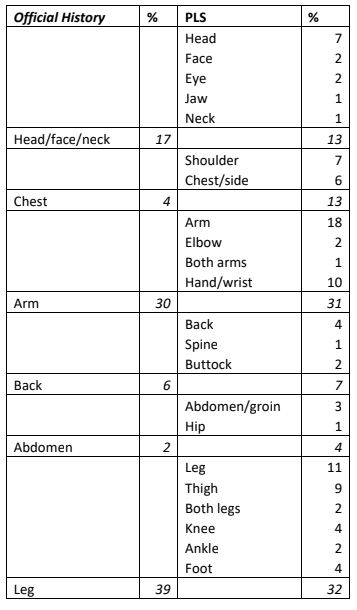
Table 14: Comparison of location of wounds in the OH (statistics)[29] and PLS
Whilst there is a concordance between the two data sets, the PLS presented refers only to gunshot wounds, whilst the OH data includes accidental ‘wounds’. The pension ledger data concerning injury is presented separately.
Whilst the OH figures add up only to 98% (the category ‘undefined’ is employed), and taking into account the caveat expressed concerning comparability, there is broad similarity between the OH hospital admission and WFA pension study data (analysis of variance yields no statistically significant difference). In the latter, more servicemen claimed a pension for chest wounds, and somewhat less for leg and face wounds, the reason for which is unclear.
In the pension ledger data, 63 per cent of the GSWs were to the limbs (69% in the OH study), which thus were, by far, the most vulnerable parts of the body. The front of the body (chest, side, shoulders and abdomen) comprised 17% of GSWs in the pension study (6% OH) with the back and buttocks making up 7% (the OH figure being similar at 6%).
(3) Multiple gunshot wounds
The pension ledgers most often detail the location of GSWs, sometimes listing up to five different bodily locations , but in a minority of occasions simply state ‘gunshots multiple’. It is unknown whether these gunshot wounds were sustained in one go, or whether all or some were sequential.
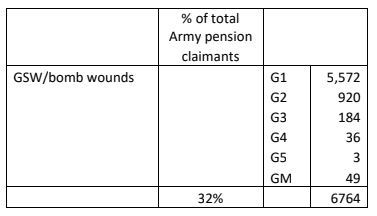
Table 15: Gunshot and bomb wounds in the PLS[number of recorded GSWs:G1 = one GSW etc. to GM = multiple GSW]
(4) Gunshot wounds leading to fractures
GSWs could leave flesh wounds (which in certain cases, e.g a gut shot, much dreaded by soldiers) might be fatal. They could also lead to orthopaedic injury.
Orthopaedic injuries were involved in 7% of cases of one GSW (G1); 5% of cases of G2; 5% of cases of G3; 9% of cases of G4; 3% of cases of G5; and no cases of ‘multiple GSW’ (although this may simply be a reflection of absent information input).
(5) The overlap between wounds and general medical conditions
As disease outnumbers wounds by a factor of 4 to 1, a significant overlap would be anticipated between the two. This in fact is smaller than expected at 4.5%.
Gunshot wounds
(A) Arms
In terms of impact on daily life in respect of GSW injuries to arms, for most jobs, proper arm flexion is required.
The final percentage disability of60 Army pension claimants with a single arm/elbow wounds only is given in Table 16. (Injuries were more or less equally distributed between right and left arms, but in terms of impairment, 90% of people are right-handed).

Table 16: Percentage disability in the two groups of 30 arm and elbow GSWs
The average percentage disability in the group with elbow wounds is 38.5%, that of the arm wound group is 28%. Perhaps unsurprisingly, given issues related to flexion, the elbow wound group were more impaired.
Seven percent of elbow GSW wounds involved fractures; as did 7% of arm GSW wounds.
GSW left forearm
- Corporal (37334) Abraham Clayton MM,23rd Battalion Northumberland Fusiliers, (who had enlisted and January 1915 and gone to the Western Front on 16/07/1916) suffered a GSW of the left forearm on 14 April 1918 (the bullet passing through), which required a ligature of the brachial artery, and his ulna was fractured. This was a comminuted fracture, i.e. the bone had broken into three or more pieces. After surgery at the Northern General Hospital, Sheffield, where fragments of shattered bone were removed, he underwent massage and passive movement (i.e. his arm was moved for him). By 14 November that year, whilst the wounds had healed, there was ‘very limited extension. No pronation or supination possible with forearm’. (The latter refers to up or down movement). There was a median nerve lesion, which was the cause of these limitations. He was ‘discharged as an invalid’ in March 1919 from Doncaster Military Hospital.[He had suffered a GSW in the neck the previous year (when he was also hospitalised with influenza), which was described as superficial, and which did not form part of his pension claim.] He was regarded first as 40% and finally 35% disabled (pensioned at 15/2d per week).He married post-war. Whilst we do not know his pre-war occupation, in 1939 he was working as a postman – any lasting effects clearly did not hamper this work. Born in 1896, he lived to the remarkable age of 96, dying in 1992.
Grenade wound right elbow
- Private (13241) John Young, Royal Scots Fusiliers, suffered a grenade wound to his right elbow which fractured his humerus (i.e. between elbow and shoulder). By June 1919 flexion was ‘good’ but extension limited. There was atrophy to the muscles of his forearm and his grip was reduced by 50% (and later improved somewhat). Pronation and supination was 50% impaired. He was rated 40% disabled and pensioned at 19/- per week. His pre and post-war occupations are unknown, but the impact on employability may have been limited.
There were only 16 soldiers in the Army series who had their only injuries as GSW to both arms or both hands. No pension records for these 16 were found. The final percentage disability recorded is presented in Table 17.

Table 17:Percentage disability in soldiers with injuries to both hands or arms
(B) Hands
To state the obvious, hands are one of the crucial features of humans adapting to life; and for the returning soldier, work.
The final percentage disability of 50 soldiers whose sole injury was a GSW hand, is presented in Table 18.

Table 18: Percentage disability for soldiers with GSW hand
Three individuals had suffered amputation, one the middle and ring finger (20% disability); one an index finger and part of the metacarpal (30% disabled); and the third middle and ring finger (40% disabled).
The pension records survive for one individual whose initial degree of disability was 20% and final disability 1%. Initially there was a ‘loss of power in little finger, grasp is poor’ in the right hand. Later there was a ‘small healed scar, middle palm’, but with injury to ‘metacarpal bone little finger’ and ‘loss of flexion’. We do not know the individual’s initial occupation (or handedness), but in 1939 he was the secretary and director of a taxi business.
GSW left hand – war and peacetime injuries combined?
- Private (4412) Frank Noakes, South Wales Borderers, a married pre-war coal miner (hewer), was wounded in July or August 1916 and discharged, aged 36. His pension ledger record states ‘GSW Lt hand, attrib 50%’ but goes on to add ‘Loss of Lt hand, non-attrib’. What had happened here? Had Noakes returned to coal mining and suffered an accident (his left forearm already bore the scar of a coal mining injury on enlistment)? In 1923 he was described as 30% disabled and pensioned at 12/- a week, a level presumably not encompassing the loss of the hand. Interestingly, and seemingly undaunted, Noakes remained in mining and in 1939, one-handed, was a colliery pumpsman (below ground).
(C) Legs
If hands were crucial to work, many jobs required the ability to stand or walk for protracted periods.
Fifty soldiers were reviewed, whose sole injury was a GSW leg, and for whom the pension ledgers gave a final percentage disability. 38% of injuries were to the thigh, 15% of injuries were to the knee, and 47% to the lower leg. Six per cent of GSWs to the thigh, knee and lower leg involved fractures. The results are presented in Table 19.
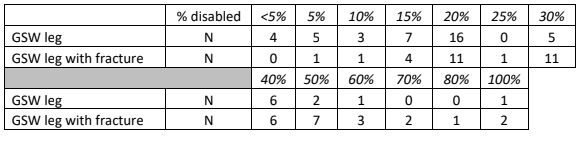
Table 19: Percentage disability for soldiers with GSW leg
The average percentage disability with a leg wound was 22.5%, but with a fracture the average disability rose to 37%. Above 40% disability involving such a fracture, all (bar one) were femur (thigh) fractures rather than tibia and or fibula (lower leg fractures).

Above: Nurses dressing wounds of leg injured serviceman, Royal Naval Hospital, Chatham (IWM Q18928)
GSW – fractured right thigh
- Private (42503) Martin Albones, Durham Light Infantry, suffered a compound fracture of the right leg due to gunshot wound to the right thigh. He also had his left arm amputated. Aged 27 at the end of the war, and single, having previously been a waggoner on a farm, now unable to drive horses, he worked as a postman. His disability was rated at 80% and he was pensioned at 32/- per week. His leg injury evidently did not hamper his chosen post-war career, which, obviously, was heavy on walking. He never married and died in 1963, aged 72.
GSW – fractured femur
- Private (295240) Alfred Watts Panter, aged 25 and married, was wounded on 20 September 1917 after two months on the Western Front with 2/4th London Regiment. As a soldier he was ‘good, steady and well conducted’. Suffering a ‘perforating wound’ to the lower end of the femur, by July 1918 his leg had healed, although it was now three-quarters of an inch shorter, and his knee could only bend 15 degrees. He ‘walked with pronounced limp’. By March 1919 the flexion had improved, and his limp was ‘slight’, but his thigh and calf showed wasting. In March 1920, flexion at the knee was now found to be full, but the wasting in his leg had worsened, and in February 1921 he complained of ‘weakness’ in the leg and the knee flexion had deteriorated. The position in March 1922 was much the same although the leg was now reckoned to be only 1/2 inch shorter. He was finally regarded as 20% disabled. He was pensioned at 8/- per week, his wife receiving 2/-. In the pre-war years he had worked as a ‘shoe hand’, and he returned to his profession, working in 1939 as a ‘boot & shoe sole cutter’. He died in 1961, aged 69.
GSW thigh and loss of testicle
- Sergeant (13/852) Ernest Good was born in 1888.At the outbreak of war he was working as a hairdresser. He had attested pre-war on 16 July 1914, serving in the 13th Battalion East Yorkshire Regiment. He had married Hannah Oliver in 1912, and the couple had three children at this point. He character being ‘very good’, he was promoted Sergeant in November 1915, and his unit went to Egypt in December 1915, thence to the Western Front. He was wounded on 15 July 1916 in the Fauquissart sector. He was evacuated to the UK seven days later, and discharged in February 1917.He was assessed as 60% disabled, and his case concluded in 1922 when he was awarded a weekly pension of 28/-, his wife receiving 17/8d. Despite the loss of one testicle, Ernest fathered another child in 1918. He did not return to hairdressing – standing may have been difficult as a result of his thigh wound. In 1939 he was working as a radio engineer. He died in 1952 aged 64.
GSW – loss of penis/testicle(s)
Ernest Good was one of a number of servicemen who injured/lost their penis or testicles to a GSW. In the PLS sample of 21,000 Army personnel, 19 men are listed as with such an impairment. Whilst such an injury might not affect employability, there are obvious ramifications of this to a full life. The marital status of four was not recorded, whereas 10 were single and five married.
- Corporal (10791) James Brydon, one whose marital status was not recorded, suffered incontinence of urine and loss of a testicle. He was rated finally as 50% disabled and pensioned at 13/9d a week. He emigrated to New Orleans and died in 1986 at the age of 92.
- Private (20077) Arthur Pateman, a single man at the time of his injury, suffered the loss of a testicle and ‘interference with micturition’ following a GSW. He was rated finally as 30% disabled receiving a weekly pension of 12/-. He married at the age of 44, his wife receiving 3/-, and in 1939 was working as a farm labourer (his pre-war job), he and his wife having no children.
- Lance-Sergeant (296951) William Edington Aitken received a GSW in the buttock and scrotum, losing his left testicle. He was rated finally as 30% disabled, receiving 13/- per week. Single at the time, and working as a chemist, he married in 1926 at the age of 32 (his wife not being added to the pension), but died nine years later, having had no children.
- Corporal (25365) Ernest Frederick Horobin lost both testicles to shrapnel. He was rated as 80% disabled, receiving a pension of 34/8d per week. A pre-war clothier’s assistant, his injury would likely not have interfered with his employment. Single at the time of his injury, he lived to the age of 80, but apparently never married.
- Private (34861) Thomas Nelson not only received a bullet wound in the testicle, he received another in the neck and the right forearm, as well as a gunshot wound in the head. The records do not exist to tell us his pre-war occupation, or his post-war fate. He was 31 at the time of his discharge, but was, rather surprisingly, only regarded as 20% disabled, entitled to a weekly pension of 8/-.
(D) Limb amputation
A minimum five per cent of gunshot wounds were associated in the pension ledgers with an orthopaedic injury. Such an injury likely increased the likelihood of amputation, and the number of servicemen recorded in the ledger sample as having undergone amputations due to GSW is set out in Table 20 below.
The OH states that .005 of all hospital admissions for a GSW resulted in arm amputation, and .01 in leg amputation. The figures from the PLS are .01 and .02 respectively in terms of all GSWs, i.e. double in both cases. Although the numbers are small the reasons for the differences are not clear. Later amputation might have occurred for some. The pension ledger figures represent 17.5% of arm GSW wounds resulting in amputation, and 7% of leg GSWs.
There are indications that 23% of the amputations may have been traumatic, i.e. whilst no doubt requiring surgery, nearly a quarter of the limbs or part limbs lost may well have been blown off by the gunshot.
495,545 men were supplied with an artificial limb, mobility aid or other surgical appliance.[30]
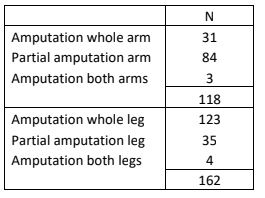
Table 20: Amputations from the pension ledger data (partial amputation represented an extremity, i.e. lower arm/leg, hand/foot, or fingers/toes)
GSW head, right thigh & arm, amputation finger
- Gunner (21215) Arthur Isaac had served in the 3rd Battalion Welsh Regiment in South Africa 1901-2, and then transferred in 1904 to the Royal Garrison Artillery, with whom he served in Hong Kong. A reservist in 1914, he was recalled and went to the Western Front on 10 August until 12 March 1915, when he returned to the UK with ‘GSW head and thigh’. His pension ledger entry shows he lost his right eye, and there was also a wound to the left arm, resulting in the amputation of his left little finger. An initial 80% disability was reduced to 70% in 1922, when he was awarded 28/- weekly. Although the ledger notes him to be single, he had one child who was awarded 7/-. On his RGA enlistment in 1904 he gave his occupation as groom – it seems likely this was not a job he was able to return to.
Amputation left leg at thigh
- Corporal (203191) Arthur Cecil Avenell was born in 1891. He was one of four brothers who served – one a sergeant-major in the Welsh Regiment, two in the Glamorgan Yeomanry, all four surviving the war. All had gone into the Army after the death of their father. Arthur, working as a painter, was the last, attesting Trooper (575) in the Wiltshire Yeomanry in 1912. He arrived on the Western Front in December 1915, was promoted Corporal in April 1917, and the following month was awarded the Military Medal. With the decreasing need for cavalry, on 25 September 1917 he was transferred to 6th Wiltshire as infantry. In terms of the overlap between wounding and disease, he had suffered contagious impetigo in March 1916, pyrexia of unknown origin in September 1916, and ‘marching feet’ with ingrowing toenails and callosities in December 1917, the latter two issues requiring hospitalisation.
At Cambrai on 30 January 1918, ‘a quiet day in front line’ so the unit war diary states, Arthur received a machine gun bullet to the left knee which shattered one of the ball shaped bones (condyles) at the end of his femur. He was x-rayed immediately and the wound was closed, although muscle and nerve damage was observed. (The third finger of his left hand was also injured). Back in the UK, by 7 February the wound was badly infected and ‘steadily losing ground’. Amputation was carried out through the middle of his left thigh on 27 February 1918, 8.5 inches below the left hip. His infection slowly subsided, but by 17 March he had pneumonia in both lungs. He would progress through seven hospitals – in June and October, pieces of necrosed bone were removed, but by 8 July his stump had seemingly healed and at the end of that month he was deemed ready for the fitting of an artificial limb. After a final period in hospital July-September 1919, during a year when his stump had broken down and was painful, he was discharged with 70% disablement. His medical journey had lasted 20 months.
He married in October 1920. Returning to his job as a painter was beyond him, and he was then working as a railway clerk for GWR at Bridgend. Awarded 30/4d a week for life, a technicality concerning his pension case would be raised in the House of Commons in 1931 (the year matters finally settled). He and his wife had five sons between 1921 and 1937, and he died on 31 December 1969, aged 78, having become a publican in Oxfordshire.
(E) Paralysis following gunshot wounds
Only 25 individuals (.001%) are listed as suffering paralysis/paresis as a result of a GSW. A further 81, however are listed as suffering such a fate without a gunshot being mentioned. Whilst clearly this injury could be acquired accidentally, it is likely that many were indeed the result of GSWs, the cause simply being omitted. Thus, a maximum of .004% of serviceman suffered such an injury.
- Sergeant (751348) Thomas Michael Athey was born in 1888. In civilian life, he worked as an electrician manufacturing switchgear for A. Reyrolle in Heburn. He was conscripted into the Royal Artillery on 16 May 1916, and on 2 July, of ‘very good’ character, was promoted Sergeant, proceeding to the Western Front the following day. He must have had leave a year later as he married on 25 August 1917. Almost exactly two months later, on 30 October, he received shrapnel in his back, chest, and left forearm. He was serving with a howitzer brigade (D317) supporting 63rd Division’s attack on Passchendaele Village – one of 11 casualties. The GSW to the back led to nerve damage and he was left with (partial) ‘paralysis and deformity left hand’. The extent of the paralysis is not known, but he was only discharged on 21 August 1918. By 1923, when his pension case was concluded, he was assessed as 35% disabled, and awarded 16/4d weekly, his wife 3/6d. A son was born in 1924. Whilst his injuries almost certainly precluded work as an electrician, in 1939 he was working as an ‘engineering progress clerk, electrical works’, likely having returned to his old employer. He was also a special constable. Thomas died in 1968, aged 80, outliving his wife by five years.
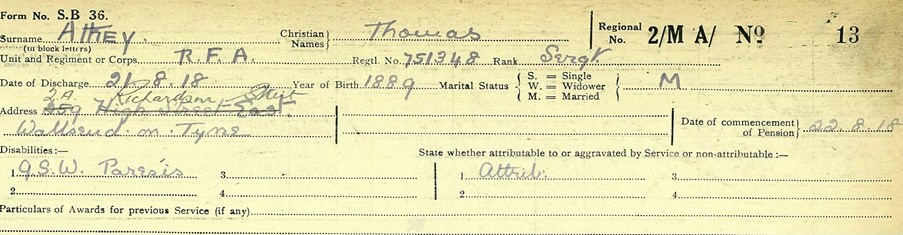
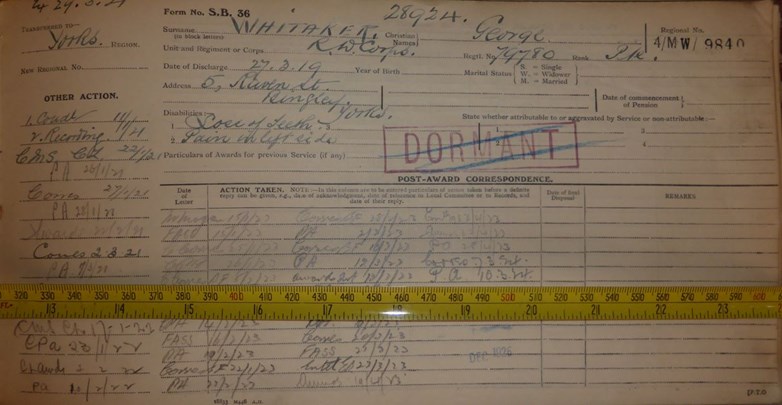
Above: The first page of Thomas Athey’s pension ledger lists his name, regiment, service number, rank, address, year of birth and marital status. His date of discharge was 21/08/1918, and his pension began on the 22nd. His condition is given as ‘GSW paresis’, and, obviously, ‘attributable’ to service.
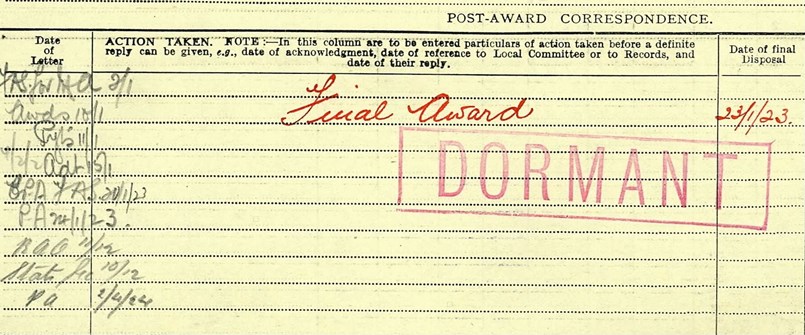
Above: On the lower part of the front page (which often gives long lists of dates of correspondence concerning the individual’s case), it is noted that a final award was made on 23/01/1923, and his case was now ‘dormant’.
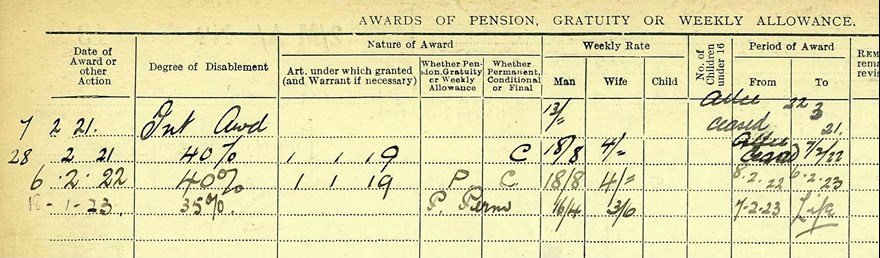
Above: The second page of the ledger notes an ‘initial award’ on 07/02/1921, Athey being deemed 40% disabled three weeks later, dropping to 35% after a further two years. His award (16/4d for himself and 3/6d for his wife) was declared ‘permanent’ on 07/02/1923 for life.
(F) Head
Seven per cent of GSWs were to the head. In the 21,000 Army pension applicants, 29 were specified as either ‘penetrating’ or leading to skull fracture (and hence possible brain injury).
The average percentage disability was 67%, ranging from 20 to 100%. A third of the injuries were associated with epilepsy, and a third were rated 100% disabled. Three suffered hemiplegia (one-sided paralysis, rated 50%, 100% and 100% disabled); one had a paralysed right leg (Private Robert Loomes, a previous Regular, married with five children, who had worked as a labourer in a Welsh ironworks, who was rated 50% disabled). Another had a paralysed right arm (80% disabled).
GSW head, fractured skull
- Private (330587) Harold Pickering, Sherwood Foresters, was 22 when he was discharged in 1918 with 100% disability, pensioned at 40/- a week. He had been wounded after three months on the Western front in 1917. On his discharge he was summarised as suffering a ‘fissured fracture’ to the right parietal region, with a ‘large trephine opening’ and ‘a great deal of bone missing’. There was slight paralysis of the hand, and he complained of headache. He had suffered epileptic fits once a month, falling backwards and biting his tongue and had to wear a protective cap. His memory was impaired, and in 1922 he was noted to be ‘nervous in traffic’, with no hearing on the side of the injury. Pre-war he had worked as a labourer, but would not work again. He never married and in 1939 was described as ‘nearly incapacitated due to war injuries, living with his parents. He died in 1961, aged 65.
Right hemiplegia from GSW
- Born in 1887, Private (7022) Ralph Frank Besant was 18 when he enlisted in 1904, Private (7022) Wiltshire Regiment, and was a reservist at the outbreak of war, a ‘skilled’ electrical labourer in the Pembroke Dockyard. He went to the Western Front with the 1st Battalion, and was very likely wounded on 13 October at La Couture, near Bethune. He suffered a penetrating head wound to the left temple (likely a frontal lobe injury), leading to right-sided hemiplegia. He had married Mary Anne Dawkins in 1908, the couple having five children. He would, of course, not return to the dockyard – his degree of disablement was 100%, and he had ‘constant attendance allowance’ of 15/- per week, the care no doubt provided by Mary Anne, on top of his pension of 40/-. A frontal lobe injury would have led to both cognitive impairment and behavioural changes. Interestingly, a son (Levison Frank) is attributed to the couple in 1917. He died at Queen Mary Hospital, Roehampton, a military hospital and the first centre for fitting prosthetic limbs, on 18 May 1936. His gravestone at Pembroke is inscribed ‘An Old Contemptible’. Sixty-four days on the Western Front resulted in 21 years of suffering, his life curtailed at 49, eventually, by sequelae of his wounds.
(G) Face
The ledger entries of 50 soldiers with their only condition indicated as ‘GSW face’ were examined.
The average final percentage disability was 35%, but this ranged from 1 to 100%. Thirteen were recorded as 50% or above disabled. The pension records of none of these individuals survive for further examination. One soldier where the ledger recorded ‘complete loss of nose’ was rated as 80% disabled.
Two ledger entries leave the observer wondering as what scale of percentage disability the assessing doctors were using. One soldier, for whom it was recorded ‘facial paralysis, disfigurement’ was rated as 30% disabled; whilst another for whom it was noted ‘deficient vision left eye, disfigurement’ was regard as a maximum 14% disabled.
Andrew Bamji, in his review of the facial surgery carried out by Harold Gillies at Sidcup, notes:
‘The vast majority of cases demonstrate that the men got on with their lives after the war. They encountered challenges and prejudice, but their children and grandchildren mostly report that they were well-adjusted and content. Where problems did occur, these issues were similar to those experienced by uninjured men … the experience of war, rather than the experience of disfigurement, was the main factor which caused post-traumatic stress.’[31]
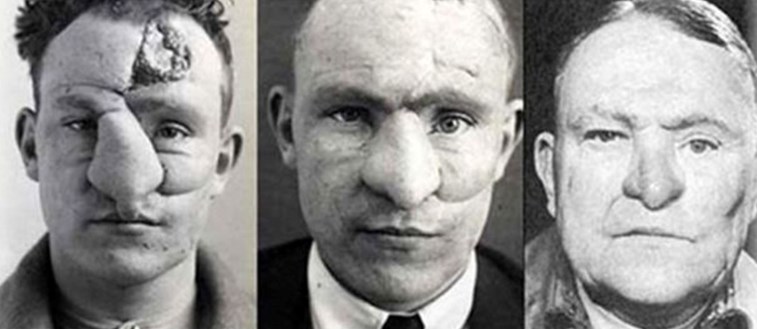
Above: Progress of facial reconstruction
(H) Eye injury/blindness
GSWs leading to blindness had a possible serious impact of post-war employment and adjustment.
Fifty per cent disability was generally assumed for the loss of/injury to one eye, and 20/- a week or thereabouts the usual pension. Of 50 Army pensioners for whom a GSW eye was the sole injury, the average disability was 55%. Two were rated at 100%, but no further information was available. One was recorded as ‘GSW eye, traumatic cataract’ (awarded 40/- per week, with 10/- constant attendance allowance, suggesting that perhaps the cataract was in the good eye); the other is only recorded as having lost a single eye, receiving the same level of pension.
- Private (35182) Wilfred Ireland, East Yorkshire Regiment, 17 at the outbreak of war, received a GSW which fractured his skull and cost him an eye. It seems inconceivable there was not brain injury. He was classed as 90% disabled in 1923, receiving 36/- a week. Married in 1921 and producing one son, in 1939 he was working in South Shields, despite his injury, as a shipyard fitter. He died in 1974 aged 77.
- Private (59358) Richard Smith Yates, Royal Scots, 15 at the outbreak of war, received a GSW which resulted in the loss of his left eye in April 1918, his final degree of disablement rated as 50% with an award of 13/9d per week. He was fitted with an artificial eye and left with a scar just above the centre of the orbital eminence. His medical records in July 1919 noted: ‘Socket healthy, slight discharge. Field of vision normal. Slight disfigurement’. Entries in his case continued until November 1924, but the following year tragedy ensued. On 17 February 1925 it is recorded: ‘Left arm and left leg torn asunder. Instantaneous death’. Despite his injury he was working as joiner, and was employed cleaning plant at the Riddochhill Colliery, Bathgate, West Lothian, when he was ‘caught by the shafting of the machinery’. Given his missing left eye and the injuries occurring to the left side of his body, one is left wondering about a possible connection, lack of peripheral vision on the left making him less aware to danger from that side.
- Corporal (24111) Cecil Joseph Ackerman, Dorset Regiment, gave different versions of his age, but was likely 19 at the outbreak of war. He married in 1916, probably before going overseas, where he suffered a facial injury and loss of his right eye. He was assessed as 50% disabled, and pensioned at 21/8d, his wife receiving 5/- a week. A dairyman before the war, in 1939 he was still in the same profession, which having only one eye clearly did not hamper. He died in 1971.
- Private (11778) John William Fox, North Staffordshire Regiment, was 23 at the outbreak of war. He received a bullet wound through the right eyebrow in December 1916 whilst serving in Mesopotamia. The eye was ‘destroyed & remains excised’. The choroid, the middle layer of tissue in the wall of his left eye was also ruptured. He was finally rated as 80% disabled and pensioned at 33/- a week, his wife receiving 18/10d. He had three children, one born 9 years after the war’s end. He worked as a potter’s dipper pre-war, and it is not known whether he was able to resume his profession, but glaze dippers, working with their hands in lead, were the highest paid pottery workers because of the dangerous nature of the job, and it might be that this task was no longer possible for him with damage to his remaining eye.
Of 21,000 Army pension ledger records, only three described a GSW affecting both eyes (although two indicate a medical problem in the remaining eye).
- Private (30817) John Henry New, South Staffordshire Regiment, was 21 when he attested in 1916, and was working as a coach trimmer. He was married with two children. After seven months on the Western Front he suffered a GSW resulting in the loss of his right eye and injury to the left. Rated as 100% disabled, he was awarded 40/- a week, his wife 23/6d. He was never able to return to his job and in 1939 was described as a ‘blind army pensioner’. He and his wife had no further children and he died in 1955, aged 61.
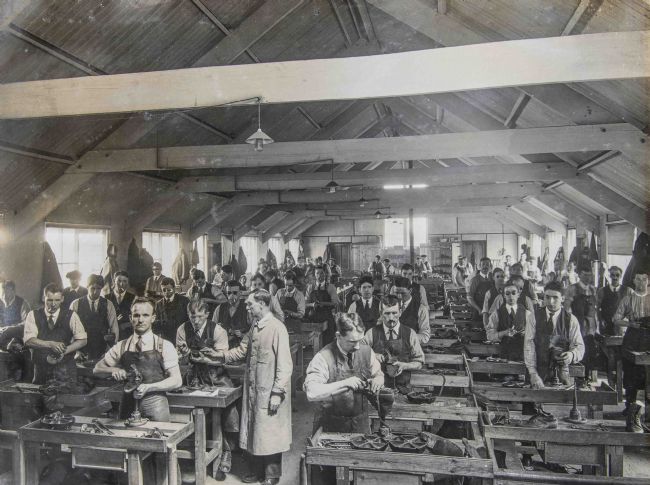
Above: Blind servicemen learning to repair boots
(I) Multiple GSW
Whilst some 49 soldiers were described as having suffered ‘multiple’ GSW, three were specifically noted to have five.
- Gunner (131234) Frederick Anker, RFA, is recorded as having GSWs to his head, both arms, buttocks and right thigh. He was judged 70% disabled at the age of 26, pensioned at 28/- per week. He had worked as a loom tenter in the cotton industry. He married in 1920 (there being mention of a pension for his wife), and in 1939 was employed as a labourer in an iron foundry, a job requiring less motor skill.
- Gunner (239970) Ellis Charles Rudd, RFA, was recorded as having GSWs to his face, forearm, hand, thigh and foot. He was, however, judged as only 20% disabled. In 1939 he was working as a grocery branch manager, having been a grocer in the pre-war era.
- Private (20593)Peter Cassidy MM, Machine Gun Corps, suffered GSWs to his right arm, toe, left thigh, right leg, right arm, and in addition lost his left eye. He was viewed as 80% disabled. No further records exist concerning him.
Thirty-three soldiers recorded with four GSWs and with evidence of % disability can be located in the 21,000 Army pensioners. What is striking is that only four are assessed as over 50% disabled. One, recorded with GSWs to skull, chest, left leg and hand was rated at only 1% disability. This is startling with the reference to ‘skull’ implying head injury. Another, recorded with GSWs to back, shoulder, arm and thigh was rated at only 5% disability; as was another with GSWs to neck, right hand, and both legs. A soldier with GSWs in the head, neck, forearm and testicles, was rated at 20% disabled. This can be contrasted to the four cases of testicular damage noted earlier, rated as nearly 50% disabled. The average per cent disability in this group is 30%.
- Private (15693) Edwin Lewis Cannon Perry, Northamptonshire Regiment, received GSWs to his right wrist and arm, and his right leg and flank. He was viewed as 50% disabled, and pensioned at 20/- per week. A pre-war clerk to a wagon builder, in 1939 he was an assistant manager in a railway vehicle repairing firm – he may well have returned to the same employer. He died in 1980 aged 86, having married, apparently for the first time, at the age of 70.
- Rifleman (14674) James Greer, Royal Irish Rifles, was reported killed in 1 July 1916, and later identified as a prisoner of war. He had suffered a GSW to the skull, both legs, and left hand. We must presume these serious injuries were cared for in Germany. Designated 60% disabled, he was pensioned at 24/- per week, his child receiving 14/-. He had been a flax rougher in the pre-war years, and it is not known whether he was able to return to this occupation.
- Gunner (21215) Arthur Isaac, RGA, was a pre-war soldier who had served in South Africa and Hong Kong with the Welsh Regiment. Having returned to civilian life, he worked as a groom. In 1915 he received GSWs to the Left thigh, arm, hand and eye, the latter being removed. Designated finally 70% disabled, and with a pension of 28/- a week, his child receiving 7/-, in 1939 he was working as a fireman in a tinplate worked, aged 56, and died in 1960.
- Private (652) Edgar Cherrington, Gloucester Regiment, received GSWs in the back, shoulder, arm and thigh in November 1914. He was categorised as only 5% disabled. A pre-war farm labourer, who has served in the 3rd Battalion since 1908, in 1938 he was employed as a cold store attendant, and died in 1964, aged 71.
Naval personnel gunshot wounds
The pension ledger records of 2,250 men who served with the Royal Navy were transcribed. Of these, it is recorded that 990 served with the Royal Naval Division. This over-representation as pension claimants is understandable given that these men served as infantry.
372 (38%) of these individuals were recorded as having sustained gunshot wounds. The numbers of number of men with single or multiple gunshot wounds is detailed in Table 21 below.
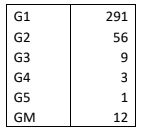
Table 21: Number of GSWs sustained by Royal Navy pensioners
It is, however, difficult to be clear exactly how many of these actually sustained their wounds in naval action. There is a discrepancy of 32 individuals between the total of Royal Naval pensioners and those known to have been in the Royal Naval Division.
There were three stokers, one deck hand, two ordinary seamen and one leading seaman amongst these 32, in addition to the three who can be clearly identified below. The remaining 22 are likely RND men who have not been identified as such in the available records.
In terms of naval actions, two individuals can clearly be identified as having been injured at the Battle of Jutland in 1916.
- Boy First Class (J/33603) Henry Robson Mallory (b. 1898) suffered a ‘shrapnel wound to the skull (hernia cerebri)’ i.e a brain injury, at Jutland on 31 May 1916, and was rated as 60% disabled, pensioned at 24/- a week. He was serving on the light cruiser HMS Castor, the flagship of the 11th Destroyer Flotilla, which was damaged by enemy gunfire. He married in 1918,and in 1939 was working with in vegetable oil processing. Mallory died in 1976.
- Stoker (SS/107602) David Tuke very likely sustained his GSW left buttock when HMS Birmingham was hit at the Battle of Jutland on the night of 31 May, causing splintering. With such an injury he was rated as only 2% disabled, paid a gratuity of £71-5-0d.
Lastly, there is one individual whose GSW remains something of a mystery.
- William Quinn, a fireman of the Mercantile Marine (908014), was pensioned for a GSW to his left leg, rated finally as 40% disabled with a pension of 16/- per week. (A note states ‘Admiralty award of £49-13-9d. per annum under Workmens’ Compensation Act cancelled). He served on HMS Mantua which was an armed merchant cruiser which served with 10th then 9th Cruiser Squadrons. It is not recorded that the ship was ever in action, although it is known for possibly striking the German merchant submarine Bremen, and having been one of the first ships to spread the 1918 ‘flu pandemic to Africa.
RAF personnel gunshot wounds
The pension ledger records of 1,750 men who served with the Royal Air Force, Royal Flying Corps or Royal Naval Air Service were transcribed.289 of these individuals were recorded as having sustained gunshot wounds. The numbers of number of men with single or multiple gunshot wounds is detailed in Table 22 below.

Table 22: Number of GSWs sustained by RAF pensioners
These servicemen were, of course, all rankers or NCOs, and were manifestly ground crew. There is only one of them who could have conceivably have flown, possible as a flight sergeant observer, and there would be no way of knowing whether he sustained the injury in the air.
Whilst we are very familiar with the transfer of injured men into the Labour Corps, this indicates a significant transfer of Army personnel, no longer fit for front line service, into the RAF.
Impact of wounds and employment
Sixty-nine per cent of wounds were to the limbs. This set in motion a decision-making process in terms of metal (more expensive initially but longer lasting) versus wood artificial limbs. ‘By the mid-1920s, more than three-fifths of artificial limbs provided by the Ministry of Pensions were made of light metals’.[32] The Ministry differentiated between ‘show’, ‘mechanical’, and ‘workers’’ limbs. The state would not provide artificial limbs to civilians until after WW2.
Physical impairment sometimes meant that men could not return to their pre-war jobs, and ‘the British government failed to provide enough resources for the retraining of the disabled’.[33] The vignettes above, however, show ex-servicemen returning to gainful employ and coping adaptively with their injuries. Although the popular image at the time of the cheerful limbless ex-serviceman was undoubtedly bogus, Jessica Meyer, in her study of the effects of impairment on masculinity observed (in her study of PIN26 files) ‘men’s insistence that they would prefer a job to receiving a pension if only they could find work’. One ex-serviceman wrote; ‘If I could get a decent job, I should not trouble about the pension’. Another wrote: ‘I am trying to make myself and family self-supporting and thereby independent of any pension’.[34] The case of an ex-serviceman miner whose right leg was amputated below the knee, and who worked down a mine for six years, indicates the degree of determination of some.[35]
Above: Limbless ex-servicemen (IWM Q 108161)

Above: Fitting a limb at Roehampton (IWM Q033686)
There was certainly a presumption made by the Ministry of Pensions that ex-servicemen ‘would seek and find work to the level of their percentage of health, the pension only acting as a supplement to a regular income’.[36] A man assessed as 20% disabled was presumed to be capable of earning 80% of his pre-war income. This may have been a reasonable assumption in an ideal world of work, but the world from 1919 onwards was far from such.
The post-war economic environment compounded the problems of reintegration into the world of employment. In 1919, over four million men had been demobilized – by late June that year the army alone had returned 112,101 officers and 2,816,964 enlisted men to civilian life.[37] The enormity of the task of reabsorption is indicated by the fact that this represented about a fifth of the workforce. Estimates based on national insurance and unemployment payments suggest that up to May 1920, seventy per cent of the unemployed were ex-servicemen,[38] a problem accentuated by civilians displaced from the war industries also seeking employment. In 1921, the British Legion claimed that 80 per cent of the unemployed were still ex-servicemen.[39] The 1920s were a period of unusually high unemployment in Britain, averaging 1.5 million out of work. In 1932, however, the number out of work reached 3.4 million, one in six of the workforce, and did not fall to two million until 1936. The Great Depression beginning in 1929, although experienced far more savagely in America than in the UK, had caused significant additional unemployment leading to homelessness and hunger, particularly in the northern industrial areas of Britain as demand for traditional products reduced. The extent of the effects of the Depression have, however, become the subject of myth. In the less industrial Midlands and Southern England, the effects were short-lived and the later 1930s were a prosperous time. As jobs were created, manufacturing of new products such as electrical goods and cars increased, and even agriculture saw a boom. Recent views on the sustained high employment of the period also emphasise the growing size of the workforce – 1.4 million individuals entered it between 1932 and 1938.[40] As younger individuals entered the arena of work in increasing numbers, veterans were bound to suffer, impaired veterans especially so. The veteran unemployment problem, however, steadily improved during the next decade. In April 1936, however, there were still 410,689 unemployed ex-servicemen, a quarter in the south and nearly a half in the north,[41] representing 22 per cent of the total of 1,895,100 people out of work that month. Bourke observes, however, that many disabled ex-servicemen at this time viewed themselves as disadvantaged in relation to the able-bodied unemployed. ‘In 1938, approximately half of disabled ex-servicemen were receiving less than the minimum award of 17s. given to single, young unemployed men without dependents’.[42]
What were the factors influencing veteran unemployment? Firstly, there were war-specific effects. Physical (or serious psychological)impairment created specific problems for employment, if not impossibility. Secondly, there were also attitudinal issues: ‘Many returning servicemen felt that they were qualified for better positions than they had held before entering the service’.[43] Thirdly, there were negative employer attitudes towards veterans. Bourke observes that employers had no incentive to give jobs to disabled men’.[44] They were a potential compensation liability as they were perceived as more likely to have workplace accidents. As one pensioner observed in an understated fashion, ‘disabled soldiers are not over popular as candidates for jobs’.[45] Another described putting in 70 job applications and only receiving one reply telling him not ‘to appear before the Committee unless I could produce a Medical Certificate certifying me absolutely fit’.[46] The Government introduced and promoted (very modern sounding) schemes whereby employers agreed that a quota of their workforce would be made up of disabled employees, but these had limited success.[47] Employer discrimination may not have been simply related to their veteran status, however, but to other features of this group, such as their age – employers were opting for younger and more adaptable individuals. Fourthly, there was the issue of general health beyond the specific impairment(not to mention the varied characters of individual veterans); and lastly, there were the compounding physiological and psychological effects of unemployment itself. The health of the unemployed is adversely affected through increase in cardiovascular disease[48] and alcohol-related conditions;[49] as well as depression.[50] The picture is not a simple one.
Gassing
The gasses deployed offensively during the Great War can be classified as:
(i) Acute lung irritants
These included chlorine, phosgene, and chloropicrin. All three had similar effects – and acute phase of asphyxia followed by pulmonary oedema. In the longer term, bronchitis and emphysema were rare, pulmonary TB extremely rare. There were occasional gastric symptoms, the commonest feature being ‘prolonged inability for severe muscular effort or even moderate exercise’, with ‘tachycardia and a rapid, shallow type of breathing’. This was ‘closely allied to the condition of disordered action of the heart’, and neurasthenia was also noted.[51] Previous bronchitis, emphysema or lung disease were risk factors. However, ‘the most severe cases may recover and be fit for duty in four to six months’, some 2-5% being permanently unfit.[52]
(ii) Vesicants – mustard gas
Mustard gas inflicted local burns, especially to moist areas – e.g. eyes and respiratory tract. Sepsis was a risk. Few cases were seen with permanent impairment of vision, and bronchitis generally resolved after six weeks. Uncomplicated skin conditions resolved within a month. Functional disorders and neurasthenia were noted aftereffects. An ‘anxiety state’ might result, the gassing layered on top of ‘Trench exhaustion, exposure to bombardment, or ill-health caused by some chronic condition such as mild trench fever, and other diseases’. Coughing, photophobia, or vomiting might be subject to ‘introspection’, and perpetuated ‘almost in a form of conversion hysteria’.[53] Disordered action of the heart (DAH) was estimated in 10% of cases, less than 3% being invalided with this a year later.[54] Functional photophobia and aphonia were noted reactions.
(iii) Lachrymators, paralysants and sensory irritants
The effects of lachrymatory gasses such as xylyl bromide or ethyl iodoacetate were smarting/burning of the eyes with burning in the throat, and generally resolved very quickly. The effects of the paralysant sulphuretted hydrogen were also temporary. Sensory irritants were arsenical compounds, such as Blue Cross. This would produce immediate and intense irritation of the naso-pharynx, and occasional transient paralysis. Large amounts were required to generate serious effects, and in most cases recovery was rapid and complete.
The Official History (diseases) states that there were a total recorded 180,983 gas casualties, with 6,062 fatalities (3%),[55] although these figures are not regarded as accurate. In 1920, 12% of total gas casualties were in receipt of pensions,[56] whilst the Official History (statistics) account of the Ministry of Pension ‘First Awards’ (made up to 31/03/1926) indicates only 1.9% of claimants awarded pensions for ‘gas poisoning’. Ina study of 2,416 examinations in September 1920 (see Table 23 below), 0.49% of gas casualties were 100% disabled, 30% disability was assessed in 16%, 20% disability in 34.7%, with 29.8% less than 20% disabled, and 11.8% assessed with nil disability.[57] The average disability was 20%. The Ministry of Pensions did not differentiate between the different gasses. (In the pension ledgers transcribed there was one reference to chlorine gas, and six to mustard gas).

Above: Gas casualties of 55th Division, Battle of Estaires, 1918.
The OH (diseases) describes a study of 150 ‘more serious’ gas cases by Colonel A. B. Soltau in March 1919,[58] where 30% were noted to suffer neurasthenia; 25% disordered action of the heart and debility; 35% bronchitis/asthma; 45% TB; 4.5% valvular disease of the heart; and 1% other complaints. Of 4,352 pensioner deaths by the end of 1920, only 1% were gas cases.
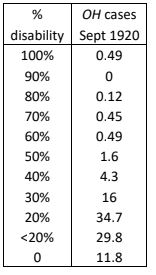
Table 23: Percentage disability in gas casualties as of September 1920 (OH)
In the pension ledgers transcribed, 558 Army servicemen (2.7% of claimants) received pensions for gas conditions. Twelve per cent of Army gas cases also had the misfortune of suffering at least one GSW.
As an assessment of percentage disability was unlikely to enhance the figures presented in Table 23 from the Official History, it was decided to examine gas cases with allied medical conditions listed in Army pensioners. Most typically, entries in the disability section referred to ‘effects of poison gas’ or some such statement, without being specific as to what this effects were.
Twenty-seven per cent of Army cases in the PLS had an additional gas-related health specifier.
- 65 cases were of gas poisoning leading to lung conditions, mainly bronchitis but with one of asthma, one of pleurisy, three of emphysema, and seven of TB. These cases had an average percentage disability of 30%.
- 16 cases were of gas poisoning leading to disordered action of the heart, with an average percentage disability of 22%.
- 15 cases were of gas poisoning leading to neurasthenia, with an average percentage disability of 19%.
- 11 cases were of gas poisoning leading to an organic heart condition, with an average percentage disability of 21%.
- 9 cases were of gas poisoning leading to debility, with an average percentage disability of 16%.
- 6 were cases of gas poisoning and burns, with an average percentage disability of 21%.
- 6 were cases of other conditions three of gastritis and three of conjunctivitis associated with gas poisoning. Laryngitis was also noted in a handful of cases.
These findings map reasonably well onto the descriptions of the acute lung irritants and vesicants described above, with half being lung conditions (none being marked as ‘aggravated’, i.e. they were not regarded as pre-war conditions). Whilst the assessing doctors predictably listed DAH, debility and neurasthenia, it is notable that in nearly 10% of cases there was an organic heart condition related to gassing, rather than a functional condition such as DAH.
- Private (268815) Vincent Walker, Sherwood Foresters, suffered with neurasthenia after gassing, likely occurring in 1917. In March 1919 it was noted: ‘Nervous, anxious expression. Rapid pulse (especially) on slight exertion, accompanied by rasped breathing. Attacks of cough & dyspnoea on exertion’. He was first rated as 30% disabled and then as 15-19%, receiving 10/6d a week, (down from 12/-, his wife receiving 7/-). Exactly a year later it was recorded: ‘Complains of shortness of breath, nervous with sudden noises. Sleep occasionally restless.’ Walker had worked as an ‘engineer’ in the Great Northern Railway, and by 1939 he was described as ‘canal labourer railway engineer’.
- Gunner (74634) Horace Edwin Marshall, Royal Garrison Artillery, was diagnosed with valvular disease of the heart related to gassing, this at the age of 24, and after only 14 weeks on the Western Front. In 1916, when he was conscripted, he was working as an undermanager in a lace warehouse where his father worked. He married in 1920, but in 1939 had no occupation, he and his wife living with his parents. He had been rated 20%, then 14% (a weekly pension of 7/6d), and it is not clear whether his lack of work was related to this or not – he was well enough to be an ARP warden. He died in 1963.
No identifiable pension records survive to illustrate a case of bronchitis after gassing in this series.
2. Injuries
The category of ‘injuries’ is problematic in terms of definition. The OH (statistics) groups injuries with disease. With reference to the ‘million card’ study, Table 21[59] refers to ‘other local injuries’ (0.5% of the total), ‘other general injuries’ amounting to just a third of the total of ‘other local injuries’. The section of this volume covering the Ministry of Pensions does not refer to injuries at all, these being presumably subsumed within the ‘other disabilities’.
In the transcribed pension ledgers, 1,377 cases out of 25,000 (6%) can be categorised as ‘injuries’. Of these, 421 (31%) were orthopaedic ( i.e. involving broken bones), 503 (36%) being soft tissue injuries. The remaining 33% were not classified, such as ‘injury right foot’ or ‘accident right hand’.
The problems which arise in these latter cases are illustrated in the following cases.:
- Bombardier (34624) John Charles Baron, Royal Field Artillery received a pension for ‘headaches caused by brick on head’ (20% disability with final of 5%). Did someone drop it on him, did it fall off a building by chance, or was there a shell explosion which dislodged it? Further, was there a skull fracture?
- Private (17009) William Ashcroft, South Lancashire Regiment, suffered an ‘injury to back and hand’, and was rated 20% disabled. This could well have been attributable to a shell explosion throwing him to the ground which did not otherwise harm him.
- Pioneer (WR/23127) John Evans, a Pioneer, RE suffered a ‘crushed right hand’, which, given his role, may well have been a labour-related injury. He was deemed 20% disabled, but we do not know whether these were orthopaedic or simply soft tissue injuries.
- Gunner (11834) John William Heatlie suffered ‘traumatic epilepsy’ (20% disability). Did a shell explosion throw him against something to hit his head, or was he accidentally struck? Again, was there a skull fracture? In this latter case we know that that 2,590 soldiers were pensioned for epilepsy but we do not know whether these cases were traumatic or idiopathic (arising spontaneously, cause unknown).
The word ‘accident’ was only applied to 15 out of the 1,377 cases. This of course does not mean that the other cases were not accidental injuries, but raises the question as to whether the injuries were in fact related to GSWs.
(i) Soft tissue injuries
Sixty-seven per cent of soft tissue injuries were hernias. When there was so much call for men to lift heavy things on the battlefield, on lines of communications and at bases, this is not surprising. However, when the cases where a hernia is listed as the first medical condition is listed, 44% are seen to be described as ‘aggravated’, i.e. the individual likely came into the army with a hernia. Again, this is not surprising given the number of civilian occupations which required strenuous labour.
- Corporal (RTS/2509) Horace Henry Coventry, Army Service Corps was a pre-war stud groom and hence was directed into the remount service, and served on the Western Front from October 1914. He sustained a double inguinal hernia (where fatty tissue or a part of the bowel, such as the intestine, pokes through into the groin at the top of the inner thigh)in the course of his work. This was successfully operated upon in January 1918, but Coventry was left with a slight left variocele (enlarged vein in the scrotum), whilst weak heart sounds, tachycardia, and deficient teeth were also noted. He was noted in his pension file to suffer debility, but the pension ledger gives the hernia as the disability. He was initially rated 40% disabled, finally 1%, and received a gratuity rather than a pension. Despite still reporting pain in his groin when he rode two years after his operation, in 1939 he was head man in a racing stables. He died in 1966 aged 83.
Gunshot wounds could resulted in hernias.
- Private Thomas Edward Longdon sustained a GSW to the right side of the abdomen on 2 July 1916 at Contalmaison whilst serving (17370) with the Wiltshire Regiment, and an associated ventral hernia (midline abdominal wall). The scar was described as weak. This did not prevent him from being transferred (275079) to the Labour Corps (UK). On 21 January 1921 he was still described as suffering ‘general weakness’. He was finally graded with a 20% disability (8/- pension per week), and the medical board discussed a belt for his hernia. He was a pre-war grocer’s assistant, married in 1920 having three children, but later became an electrical engineer. His war injuries appear not to have handicapped his work, and he died in 1966 aged 72.
Other soft tissue injuries included sprained ankles/wrists/hips/backs and spines; knee cartilage injuries (often referred to as ‘internal derangement’); and contusions of various parts of the body,
- In the case of Private Alexander Stephen, his pension ledger records ‘contusion chest (buried)’ He sustained this injury serving with the Black Watch (201836) and was transferred as a result of the injury injury to the Army Ordnance Corps (041684). He was awarded a £5 gratuity, but no pension. It may be imagined that such cases were not uncommon.
- Lance-Corporal (37419) Henry Frazer, Northumberland Fusiliers, was another such case. He was diagnosed with 20% disability as a result of ‘sprain left knee (buried in trench)’.
- Rifleman (15/1048) Thomas Jones, Royal Irish Rifles, sustained a contusion to the left arm but with ‘functional paralysis (i.e. not organic in origin). He was rated finally as 20% disabled.
- Very occasionally a case such as that of Private (2137) Joseph Osborne Grove, Warwickshire Regiment, is encountered, where contusion is recorded alongside a wound. He suffered a wound to the right side of the head with a contusion to the right eye. He was classed as 50% disabled, his weekly pension being 20/-, his wife receiving 11/9d per week.
- Sergeant (2558) Sidney Edward Bentley DCM, Northumberland Fusiliers, similarly suffered ‘contusion of eyes’, mechanism of injury unknown. He was granted a £5 gratuity, but no pension.
- Sapper (28936) Patrick Fallon RE clearly suffered soft tissue injuries which led to sequelae, given as ‘rheumatism following fall’ (20% disability).
- Lance-Corporal (9160) Edward Blastland, Lincolnshire Regiment, had the misfortune to suffer a GSW to the face, but his first listed injury was ‘wounded by pick, right hand’. Initially classed as 50% disabled, his final disability rating was 6-14%.
(ii) Orthopaedic injuries
Thirty (7%) of the orthopaedic injuries were dislocations, the remaining 93%being fractures. Seventy-six percent were either upper or lower limb fractures.
Limb fractures must have been common in labouring workplaces in this era. In the Second Report from the Select Committee in Accidents in Coal Mines (1854), 71% of non-fatal injuries were to lower and upper limbs. To prove nothing had changed, one mining company’s injuries 1945-6 reflected 72% limb injuries.[60]
It is possible that some of these injuries are the result of GSWs, which are not recorded. Private (3003) Thomas Rower Eastgate, Royal Fusiliers, however, acquired a fractured mandible via a kick from a horse (15-19% disability).
A number of spinal fractures were recorded, with no reference to paralysis.
- Private (21441) Luther Fitzgerald Brown, Somerset Light Infantry, suffered a fractured spine. Initially regarded as 100% disabled, his final disability rating was 50%. He married in 1924, and died in 1971, aged 83. A clerk in the pre-war era, in 1939 he was working as a production clerk in a coach building work. His injury had not impeded his employment.
A skull fracture might well lead to brain injury, but in the absence of imaging techniques, such may have gone unrecorded.
- Private (5950) James Gallagher, Royal Irish Rifles, clearly sustained a serious head injury with compound factures of the skull. He was rated as 100% disabled and awarded a pension of 40/- a week for life, with 35/6 for his wife and six children. His pension records do not survive to shed further light on the details of his condition.
- Private (19028) Bert Fower, Suffolk Regiment, suffered the exact same injury. Rated at worst as 70% disabled, his final rating was 50%, with a pension of 20/- for life. His pension records, similarly, have not survived.
- Private (915) John Hill. Leinster Regiment Suffered a fractured skull with associated deafness, his disability assessment dropping from 100% to 80%, with a 32/- pension. His pension records do not exist.
In one case in this series, the brain injury is obvious, but not recorded:
- Private (13/18908) Alfred Oldham, Sherwood Foresters, was nearly 36 when he enlisted in November 1914. He was a plasterer by trade. He served on the Western Front for nearly two years before being invalided to the UK in July 1915 as a result of ‘age and mental disturbance’. It was later recognised that hat these were the effects of a skull fracture, and estimated at 40% disabled. No further details are known about him.
3. Medical conditions
The medical conditions recorded as pensionable in the ledgers offer one important feature – they record whether such are ‘attributable’ to war service or ‘aggravated’ by war service, i.e. whether the serviceman brought that condition with them into the services. This reminds us of the intimate relationship between illness due to war service and general public health.
The health of the general population and recruits
Life expectancy had undergone a sharp improvement from the mid-1870s, and in 1911 the average male lifespan was 51.5 years (that for women being 55.4).[61] This had been achieved largely due to health improvements in the young population, infant mortality in particular falling. Improving health, leading to greater longevity, naturally led to increased exposure to diseases of ageing. The end of the 19th and start of the 20th centuries saw ‘an epidemiological transition in which the primary causes of mortality shifted from infectious to degenerative, or age-related diseases’.[62] There remained, however, the problems of urbanisation and associated poor living conditions, which affected those of all ages. Infectious disease had been reduced by the rise of hospital medicine, vaccination and improved sanitation, not to mention improvement in nutrition. There were no more large-scale cholera or typhoid outbreaks, and smallpox and typhus were in retreat. Tuberculosis, whooping cough, diphtheria, scarlet fever and measles – associated with poverty and overcrowding – were still rife, however. At the start of the 1900s infectious disease still caused a third of all deaths.[63] Due to increased incidence of disease related to aging, prevalence of sickness, defined as the amount of sick-time experienced by the population at risk over a given time period, increased as the 1800s progressed.[64]
Army recruits in the late 19th and early 20th centuries ‘have been shown to be broadly representative of the working class’. And contrary to some contemporary opinion, there is evidence, taken from analysis of mean height of recruits, that ‘health and strength … seems to have risen gradually during the late 19th century’.[65] Despite these improvements, in recruitment in 1898, of the ‘number of men served with notice papers’, totalling 84,626, just over 38% were rejected. The superintending officer of recruitment for the London District remarked just over 20 years earlier, when the rejection rate was 22%: ‘If I were to try to find out too much, the recruiting would fall off very materially’. Medical officers could not be ‘too fastidious’.[66] It is difficult to be exact about the causes of an increasing rejection rate during a period of steadily (if slowly) improving health. Nearly half of volunteers for the Second Boer War failed to reach the required standard. This increased preoccupations with degeneracy, and gave ‘strong impetus to the Liberals’ programme of domestic reforms from 1906’.[67]
Men from the Dominions, notably Australia and Canada, have traditionally been seen as:
‘Hardy, vigorous, strong … untouched by the moral and physical degradation of England’s “dark satanic mills”’, yet ‘far from being straight-backed and muscle-bound northern supermen, the majority of CEF members had decidedly unimposing physiques. Moreover, a significant number of CEF recruits suffered from a wide variety of health concerns that ranged in severity from minor to serious’.[68]
Clarke et al’s study of enlistment records of 20,000 Canadians showed that ‘many suffered from a wide variety of health concerns ranging from poor eyesight and dentition through to serious musculoskeletal, neurological, and psychiatric disorders. Moreover, evidence suggests that many recruits were poorly nourished’. In respect of the latter problem, service was beneficial – men put on 2.7kg on average whilst wearing khaki. In the winter of 1914–15, among Canadian soldiers on Salisbury Plain, 222 per 1,000 per annum were reportedly infected with venereal disease. (Among Australian troops in Britain, the rate of infection ranged between 134 and 148 per 1,000 per annum).
One interesting study of British workers of the period informs us further, particularly in relation to the effects of the urban environment on health. In their review of the health of postal workers in the second part of the 19th century, Brown et al[69] describe ‘the urban penalty’, the ‘London/urban’ group generating most sickness, ‘town’ generating half as much sickness, and ‘rural’ least. Perhaps surprisingly, poor mental health was the fourth (joint) most frequent pensionable condition, with 60% of individuals pensioned for this reason living in London. 14.1% of postal workers were so pensioned (in comparison with 3.6% of police pensioners at this time, which may reflect differential job selection). Orthopaedic issues were the most frequent pensionable conditions, an occupational issue with workers walking long distances. The second and third most frequent causes of pension claims were respiratory followed closely by consumption (TB – although the police were more prone to being pensioned for this condition that postal workers, 12.7% of pensions as compared with 7.6%). ‘General debility’ came joint fourth with psychological conditions. Visual problems came fifth, indicating perhaps another occupational issue, employees working in poor lighting conditions until the end of the century when electric lighting was installed. Digestion and cardiovascular/circulatory problems were more evident in Londoners, although digestive conditions were the least most frequent of nine groups of conditions. What this fine study fails to show, is the overlap of multiple conditions.
Health and recruitment 1914
In August 1914 the following guidelines were issued to examining medical practitioners in terms of the principal points in the medical examination of recruits:[70]
- That the recruit is sufficiently intelligent;
- That his vision, with either eye, is up to the required standard;
- That his hearing is good;
- That his speech is without impediment;
- That he has no glandular swellings;
- That his chest is capacious and well formed, and that his heart and lungs are sound;
- That he is not ruptured in any degree or form;
- That the limbs are well formed and fully developed;
- That there is free and perfect motion of all the joints;
- That the feet and toes are well formed;
- That he has no congenital malformation or defects;
- That he does not bear traces of previous acute or chronic disease pointing to an impaired constitution;
- That he possesses a sufficient number of sound teeth for efficient mastication.
General conditions of rejection:
- Indication of tubercular disease;
- Constitutional syphilis;
- Bronchial or laryngeal disease;
- Palpitation or other diseases of the heart;
- Generally impaired constitution;
- Under standard of vision;
- Defects of voice or hearing;
- Pronounced stammering;
- Loss or decay of teeth to such an extent as to materially interfere with efficient mastication;
- Contraction or deformity of chest or joints;
- Abnormal curvature of spine;
- Defective intelligence;
- Hernia;
- Haemorrhoids;
- Varicose veins or varicocele, if severe;
- Inveterate cutaneous disease;
- Chronic ulcers;
The recruit having, if possible, had a bath or been washed, and being wholly undressed, the following should be the order in which the examination is carried out:
- He is measured under the standard;
- He is weighed;
- His chest measurement is taken;
- His vision is tested.
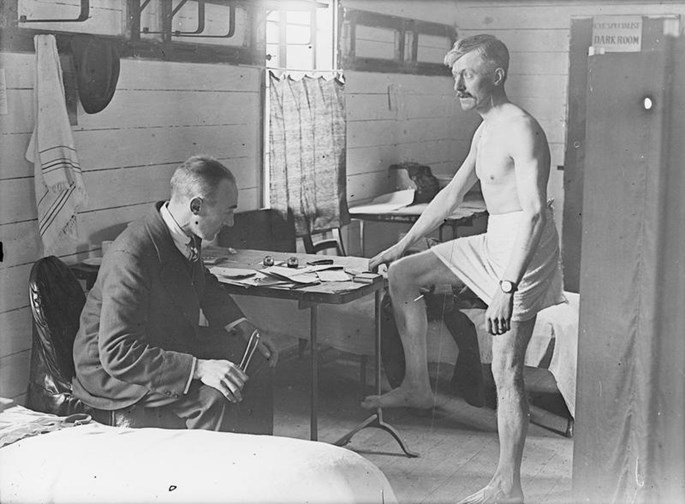
Above: Army medical examination (IWM Q 30062)
John Tucker wrote of his medical examination in November 1914. He was ‘under age … and had a disability in my rib-cage’. ‘I took off my jacket and was told to hold out my arms, open and close my fingers; the MO said OK and turning on his heel walked off. No stethoscope was used and no pulse rate taken’ He described the proceeding as ‘farcical’.[71] Ilana Bet-El describes medical examinations as ‘notoriously superficial throughout the war’ (at least up to 1917), noting that the civilian doctors employed in 1914-15 were paid ‘one shilling for each man they passed, and nothing for men they rejected’.[72] In the conscription era they were paid per session, but were still subject to time pressure. It seems highly unlikely that any detailed examination/history taking for the conditions above could have been carried out, although attestation papers indicate that the four issues of height/weight/chest girth/vision were taken and recorded with some general observation about physical appearance/health (and vaccination status) made. One 1916 conscript with colitis was told he could not be rejected, but would have to apply to a board for exemption – ‘They are accepting almost anybody now: cripples, men with hernia etc.’ he noted.[73]
The Official History (medical) notes that the influx of volunteers in 1914 required a matched influx of civil medical practitioners and that ‘the most diverse results were obtained, and many men were admitted into the army unfit for general service’.[74] Although ‘many were discharged before joining a draft for overseas, a certain number’ went on active service where they proved ‘a serious encumbrance’. Many of these medical problems ‘were sufficiently pronounced to have been detected at the time of the medical examination’, and the OH goes on to refer to ‘inexperienced civil examiners’, before acknowledging the likely real reason ‘in many cases’ due to these doctors ‘attempting to inspect more recruits in a day than could be examined properly in the time’. In December 1914, this rate was limited to six or eight in an hour, or 30-40 in a day. Problems persisted and there was a push for uniformity in assessment from March 1915, with standing and travelling medical boards. By the end of 1916 only 6.5% of new recruits were rejected, with approximately 50% graded A1. In 1917 procedures were further changed to a much greater degree of thoroughness – a conscript from late 1917 describing filling in a ‘double quarto sheet’ of history, and ‘was X-rayed and had an electrocardiogram taken … I was then tested for blood pressure etc. – had to whizz up and down stairs and then had my pulse felt’.[75]
'War syndromes’ – medically unexplained symptoms
The following review of physical medical conditions in the PLS covers conditions which are palpably organic in nature. It also covers those which are regarded as ‘medically unexplained’.
Jones and Wessely note that ‘controversy has raged over the nature of particular post-combat disorders such as shell shock, disordered action of the heart (DAH), effort syndrome’ etc, arguing that they should be classified as ‘functional syndromes characterised by medically unexplained symptoms, which include: fatigue, weakness, sleep difficulties, headache, muscle ache and joint pain, problems with memory, attention and concentration, nausea and other gastrointestinal symptoms, anxiety, depression, irritability, palpitations, shortness of breath, dizziness, sore throat and dry mouth’. [76]
Considering the influence of psychological issues of these matters, they draw a distinction between psychiatric diagnosis of Post-Traumatic Stress Disorder, whose hallmark is traumatic recollection and avoidance, and ‘functional somatic syndromes such as irritable heart or DAH which are defined by the presence of multiple, clinically significant somatic symptoms’, in the absence of the symptoms. Somatic disorders (i.e those where the individual focusses excessively on certain physical symptoms), they note, ‘are associated, but are not synonymous, with anxiety and depression’. They suggest that these somatic symptoms are culturally determined by health preoccupations (e.g. the concern about peptic ulcers during the period of WW2 and the frequency of gastrointestinal symptoms in soldiers of that period).
Jones and Wessely studied (with a careful methodology) pension files from the Boer War, the First World War, the Second World War, and more recent conflicts (N=1,856), with symptoms reduced to the 25 most common. Cluster analysis identified three syndromes (i) a debility cluster (N=575);[77] (ii) a somatic cluster (N=434)which was indicative of a functional cardiac syndrome;[78] and a neuropsychiatric cluster (n=575).[79] In the Boer War sample were 200 cases of DAH, and 200 of rheumatism. In the First World War sample were, similarly, 200 cases of DAH, 200 of neurasthenia, and 167 gassed cases. The Second World War sample included 67 cases of effort syndrome, 200 cases of psychoneurosis, and 100 of dyspepsia. Debility syndrome was largely related to Victorian, Boer War and First World War cases. Somatic syndrome was largely comprised of First World War cases; and the neuropsychiatric cluster was predominantly composed of Second World War and later conflict cases.
Overview – the pension ledger study data on medical conditions
Medical conditions and injuries were a far more frequent cause of hospital admissions during the war, existing in a 4:1 ratio to wounds (see Table 5). Pension claims for medical conditions made up two-thirds of the total pension claimants in the pension ledger study. Men also claimed for more than one condition (up to five - M1-M5 in Table 24), some 22% of ‘medical’ claimants presenting multiple conditions.
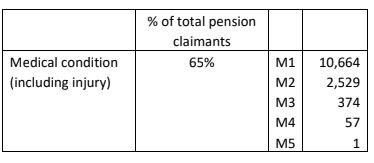
Table 24: Number of claimants in the PLS for single and multiple medical conditions
Tables 25 (a) & (b)on the following two pages present the main medical conditions abstracted from the pension ledgers.
The most prominent medical conditions pensioned (expressed as a % of the 25,000 claimants) were:
Malaria 8.3%
Bronchitis 6.4%
Disordered Action of the Heart (DAH) 5.6%
Rheumatism 5.6%
Valvular Disease of the Heart (VDH) 4.5%
Pulmonary tuberculosis (TB) 4.4%
Debility 2.8%
Myalgia 2.7%
Deafness 2.4%
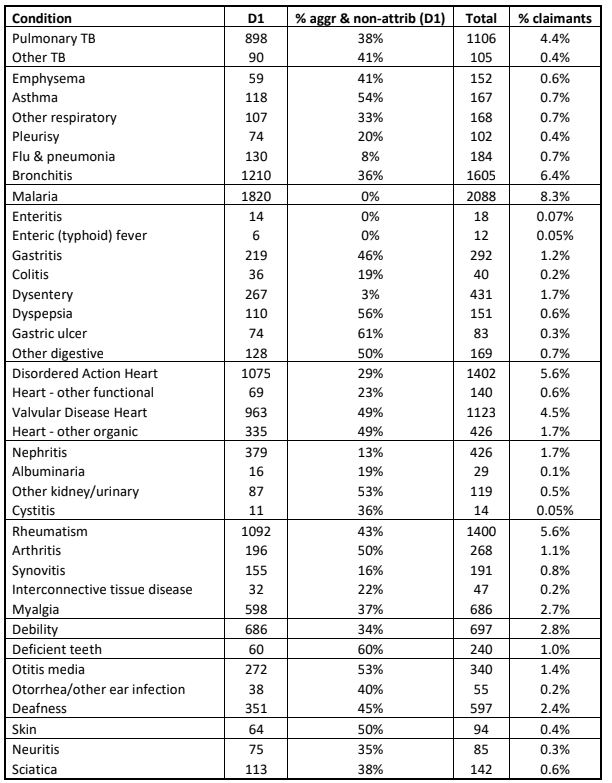
Table 25a: Medical conditions in the PLS (D1 = first listed condition)
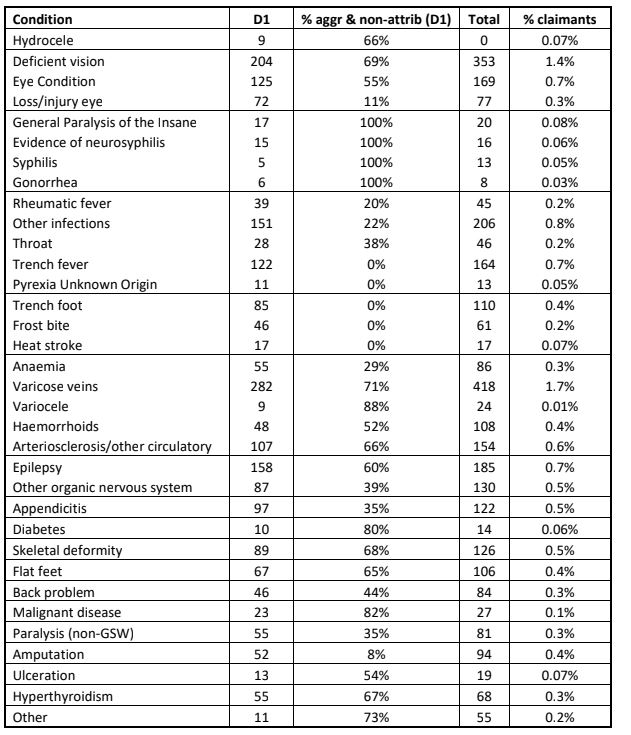
Table 25b: Medical conditions in the PLS (D1 = first listed condition)
Malaria
Malaria was the most frequently pensioned medical condition in the PLS, 8.3% of claimants being awarded a pension for this illness. Malaria was a condition prominent in first awards 1920-21, but decreased significantly over time – it demonstrated little latency.

Above: Draining marshes to prevent malaria (Open Government Licence, v 2.0)
Overview
The Official History (diseases) confirms this picture, stating: ‘Of all diseases responsible for casualties during the war malaria probably holds first place’.[80] Macedonia holds ‘first place’ amongst the locations in which service personnel fell victim to the disease – 160,000 hospital admissions alone in this location occurring 1916-18. The true number of those actually infected will never be known. During the 1918 ‘flu pandemic 83 out of 100 men autopsied in Macedonia showed signs of malarial infection without having been an active case – ‘This figure therefore would probably not be too high an indication of the percentage of the army which actually became infected’.[81]
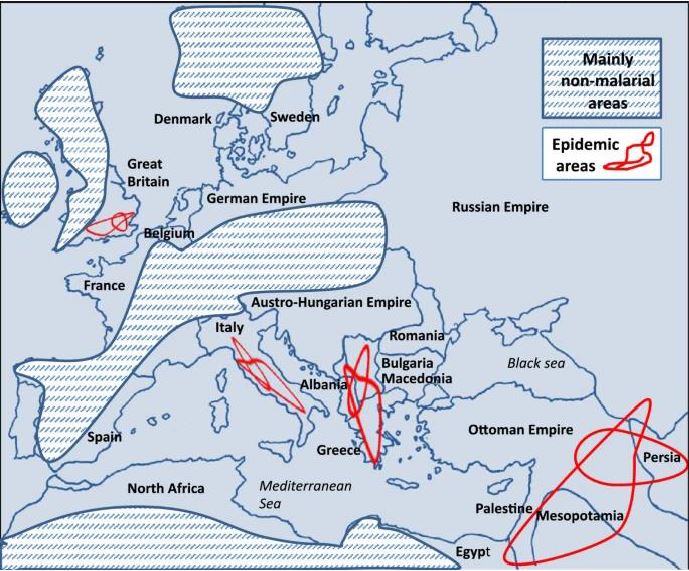
Above: Malaria epidemic areas WW1[82]
In the ‘million card’ study, 33,903 cases were identified, but, again, these figures pertain to hospital admissions. In the OH (statistics), malaria made up 7.6% of Class II (stabilised) cases and 0.5% of Class III (unstabilised) cases. In stabilised cases, in terms of ‘disease’, only neurasthenia ranked higher. 43,197 stabilised awards were made for malaria by March 1929. Between 1920 and 1926, 23,799 first awards were made for malaria, the next lowest figure being 12,574 for TB.
Signs and symptoms of malaria may include: fever, chills, headache, nausea and vomiting, diarrhea, abdominal pain, muscle or joint pain, fatigue, rapid breathing and heart rate, and coughing. Some people who have malaria experience cycles of malaria ‘attacks’. An attack usually starts with shivering and chills, followed by a high fever, followed by sweating and a return to normal temperature. Sequelae might include marked wasting and anaemia. Mortality is high in severe malaria, and cerebral malaria leads to significant brain damage.
Malaria in the pension ledger study
In the PLS, 2,088 cases of malaria were recorded (8.3% of cases). Co-morbid dysentery was noted in 4.4% of cases of malaria.
In a series of 60 cases where malaria was the sole diagnosis, the average final disability level was 19%, i.e. comparatively low. Just under half of the sample was rated at 20%, the lowest level of disability rated at 2%, the highest at 70%, this being the only case rated at over 50%.
The following case demonstrates the fluctuating pattern of malarial attacks:
- Driver (T2/13217) Joseph Bolam RASC was either 22 or 23 when he attested in September 1914. He was described as a labourer and his physical development was described as ‘good’. His malaria was first diagnosed in August 1917, degree of disablement being 50% as of August 1919. He was then described as ‘well developed & nourished, spleen tender and enlarged, sallow complexion, no anaemia, tongue fairly clean.’ In March 1920 it was recorded: ‘Has had 4 attacks since Aug 1919, last one a week ago lasting 1 day, no sickness, no prodroma’ (i.e. warning symptoms), ‘no anaemia, no cachexia’ (wasting). ‘Liver and spleen normal’. He was now viewed as 15% disabled. In March 1921 it was noted: ‘Last att(ack) two months ago, shivering, sweating lasting 1 day – 5th attack since March 1920.’ Now rated 20% disabled, his blood was screened (in his case negative for malaria parasites) and treatment commenced. This would have been quinine treatment (in such a late case, orally for a minimum 21 days. This treatment was associated in some cases with tinnitus, visual problems and mental confusion). In August 1921 it was noted ‘had attack 6 weeks ago’, by which time he was viewed a 6-14% disabled, receiving 7/6d a week.
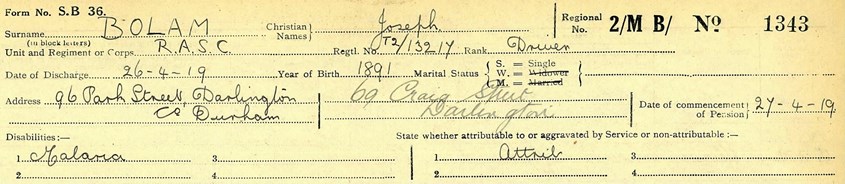
Above: The first page of Joseph Bolam’s pension ledger shows his name, regiment, service number, rank, year of birth and marital status, as well as two addresses. His condition, malaria, was noted as ‘attributable’. It states that he was discharged post-war on 26/04/1919, his pension commencing on the 27th. Below it is noted that his award was made final on 03/04/1922, and his case was now dormant.
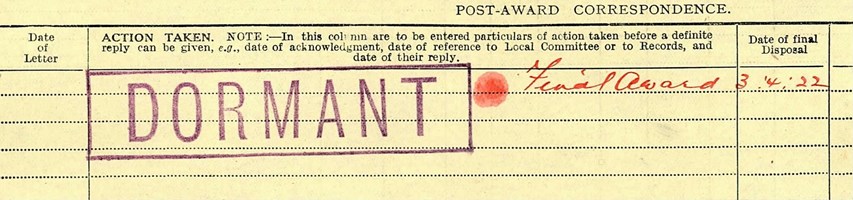
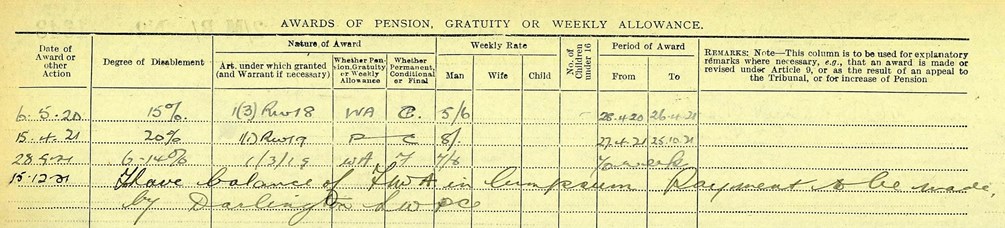
Above: The second ledger page does not show the August 1919 assessment of 50% disabled indicated in his surviving pension file, but the fluctuating ratings 15% (06/05/1920); 20% (15/04/1921); and 6-14% (28/09/1921). It will be observed that the end of the periods of award coincide with reassessment, and that Bolam’s last assessment awarded him 7/6d for 70 weeks, and that the balance of the final award was paid as a lump sum on 15/12/1921, ten weeks after the final assessment of 70 weeks was made.
A similar pattern of fluctuating disability levels, no doubt related to continued attacks, is seen in the following case:
- Private (DM2/170469) John George Curry (Army Service Corps) demonstrated an interesting pattern of disability assessments in relation to his malaria. In January 1920 he was rated as 20% disabled (8/- per week). A year later in February 1921 he was rated as 40% disabled (16/- per week), although four months later in June the rating had dropped to 30% (12/- per week) achieving a similar rating in December that year. and dropping back to 20% disability in November 1922. This reflects, one imagines, a significant upsurge in the condition a minimum 24 months after he returned home to the UK with the disease. He had previously been an infantryman, and it seems likely his transfer to the ASC was health related. He died in 1932 aged 41, and as his malaria was not severe, his demise may well not have been related to his illnesss.
A similar case is that of:
- Private (16143) David Richard Bowen served with 8th South Wales Borderers, accompanying them to Salonika in November 1915. He was discharged in January 1919 with malaria from the 3rd Battalion, so clearly he had previously returned to the UK. In August 1919 he was rated as 20% disabled, but a year later as 50%, this his final award, aged 24. He died in 1953 having worked as a turbine driver in a power station, having retired on ill-health grounds in 1951.
Even in cases with conditions associated with malaria, disability ratings are low:
- Corporal (50011) Alfred Greenwood Beavis who had anaemia as a consequence of his malaria was regarded as 20% disabled.
- Sapper (164199) James Addis suffered both malaria and dysentery. Rated as 30% disabled in 1920, in 1923 he was rated as 6-14% disabled.
- Lance-Corporal (96334) George Henry Addison had both malaria and tachycardia, and was rated as 20% disabled in March 1921, and as 6-14% disabled 18 months later.
Respiratory conditions
Respiratory conditions were recorded in 3,484 servicemen, comprising 14% of all pensioners, and were the first-listed condition of 2,596 men (10% of all pensioners). Table 26 shows the distribution of such conditions.
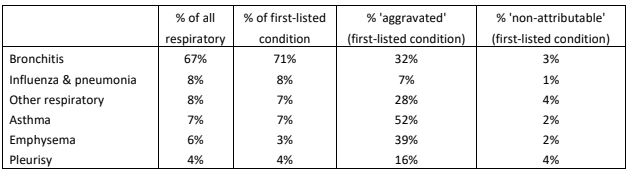
Table 26: Respiratory conditions as recorded in the pension ledgers as percentages of all respiratory conditions, and first-listed respiratory conditions, with percentages of first-listed conditions ‘aggravated’ by the war.
Influenza/pneumonia and much of the pleurisy would have been acute onset infection-related, and it is thus not surprising that these conditions were the lowest-rated as ‘aggravated’. The fact that 54% of asthma and 41% of emphysema conditions were regarded as ‘aggravated’ or ‘not attributable’ is notable. The latter is largely caused by airborne irritants and would have almost certainly been largely employment-related. Asthma has a wider range of causes (genetic, infection during early development, allergy-related, and environmental factors – many of which at this time would also have been employment-related. Occupational asthma is currently the most prevalent occupational lung disorder in industrialised countries).
Two case studies illustrate the interaction between sensitisation to asthma in previous employment and aggravation by war service:
- Shoeing Smith (101707) John Aherne, was a blacksmith farrier in civilian life, and was 45 when he attested in December 1915. He obviously continued this trade in the Army, did not serve overseas, and was discharged physically unfit in January 1918. On attestation his chest expansion did not give cause for concern, and he was viewed as ‘fit for service at home and abroad’. In 1920 he was viewed as 50% disabled, reduced to 30% in 1922 (Pension of 12/- weekly), and the summary of his conditions were ‘asthma, emphysema, obesity & age’, described as ‘aggravated partly & constitutional’. Exposure to smoke and dust over a forge would have likely been the cause of his asthma, as well as irritants from metal. This would have only been compounded in his army work.
- Sapper (146141) Harry Ramsay was 25 when he attested in November 1915. A joiner by trade, who worked in HM Dockyard Rosyth, he was assigned to the Royal Engineers, and for seven months in 1916 was released for munitions work. He did not serve overseas. There was nothing of concern with his chest expansion on attestation and he was passed as of ‘fair’ physical development, and ‘fit for field service home & abroad’. His health deteriorated during 1917 and he was discharged in October that year. Rated at 30% disabled in 1919, he was diagnosed with asthma ‘aggravated by service’. As a joiner, sawdust was a likely cause of his asthma, which would have been worsened by fumes in munitions work.
Bronchitis
Bronchitis is an infection of the main airways of the lungs (bronchi). Symptoms include coughing up sputum, wheezing, shortness of breath and chest pain. The condition can be acute or chronic. In more than 90% of cases the cause is viral, spread by coughing or direct contact. Between 1838 and 1920 bronchitis made up 8% of deaths, second only to pulmonary TB (9.8%). Its incidence increased rapidly up to 1880, due to overcrowding, urbanization and industrialization. Coal-related smogs may have been a major issue (these decreasing in line with the fall of bronchitis-related deaths from 1895).
The Official History (Statistics) does not consider bronchitis on its own, lumping it in with all forms of respiratory conditions. This is because ‘hospital return never made a reliable differentiation between purulent bronchitis and other respiratory diseases’. The Medical Services volume concerned with Diseases notes that ‘respiratory affections were common, and at certain periods the numbers affected were large, more especially during the cold and wet seasons’.[83]Catarrhal, muco-purulent and frankly purulent types were noted, but also an acute purulent type, seen mainly in the winters of 1914 and 1916.
Chronic bronchitis is long-term inflammation of the bronchi. It is common among smokers – an almost universal habit and encouraged at the time. People with chronic bronchitis tend to get lung infections more easily. They also have episodes of acute bronchitis, when symptoms are worse.
Bronchitis was the second most frequently pensioned medical condition in the PLS, comprising 6.4% of awards. As Table 26 shows, bronchitis comprises two-thirds (67%) of all respiratory conditions (46% if pulmonary TB – see below – was included as a respiratory condition). The pension ledgers are unreliable in nomenclature (acute v. chronic), but we can assume that they by and large refer to chronic cases. Thirty-two per cent were described as ‘aggravated’ and three per cent as ‘non-attributable’. Thus a third of men had bronchitis on entering the Army. The rate in the Army was 6% of pensionable conditions, 5% in the Navy, and 7% in the RAF.
Fifty randomly selected cases were examined where bronchitis was the sole diagnosis. Twenty were rated as aggravated. The average disability ratings were not high, at 23%. One case was rated at 60% and three at 40%, but 11 were rated as below 20%. Interestingly the ‘attributable’ (range 60% to 5%) and ‘aggravated’ cases (range 30% to 10%) had exactly the same average disability ratings (23% for both). There does no therefore seem to be discrimination by examining doctors against cases with a pre-war history.
- Private (384069) Bartholomew Brown, initially Seaforth Highlanders and later 13 and 296 Labour Company, was diagnosed with ‘chronic bronchitis’, attributable to service. He was rated finally as 20% disabled. Born in 1878, he attested in August 1914, giving his age as 27 (he was 36), at which point he worked in an industrial setting as a hammerman. His physical development on enlistment was described as good, and he was married with five children. He went to the Western Front in May 1915, and was hospitalised for six days in December 1916 with bronchitis (invalided to the UK), when it was stated that ‘He says he never had bronchitis until he was at Arras in 1916; he has had several attacks since, and has never been quite well.’ He was hospitalised again in February-March 1917 for 20 days. He appears to have been transferred to the Labour Corps in August 1917, having returned to the Western Front that May. In July 1918 he was hospitalised again as a typhoid contact but actually with pleurisy, and again in January 1919 with bronchitis once more. He was discharged with the following description; with a ‘pale face’, he was ‘breathless on exertion & has a cough. General wheezing’. He was 60% disabled at this point, but obviously improved. He was pensioned at 5/6d a week each child due 4/10d.
- Private (82692) John William Barker was a labourer who was nearly 28 when he attested in December 1915. On examination his chest expansion (one inch) was less than most. (Two to five inches is normal, and less would be taken as highly possible lung/pleural disease). Any previous history recorded was limited to a foot injury, however, and he was described as having ‘good’ physical development. He was mobilized in October 1916 into the Royal Army Medical Corps, and served until August 1918, when he was discharged as unfit. ‘Steady, honest and reliable’, he was rated as 15% disabled in April 1920 (5/6d per week), his bronchitis aggravated by service, his level of disability reduced from 40% on discharge. At discharge it was noted ‘Cough especially at night … night sweats, occasional haemoptysis’ (coughing up blood). More serious illness was discounted – ‘No TB in sputum’. In April 1920, ‘loud harsh respiration’ was noted, with a ‘murmur’ in the apex of the left lung. His bronchitis was dated to 1909. In 1939 he was working as a mineral water salesman.
Cardiac conditions
The cardiac conditions listed in the pension ledgers are split between ‘organic’ i.e. where there is something structurally wrong with the heart, and ‘functional’, where there is abnormal function rather than a structural fault. Functional heart disease demonstrated little latency, being one of the prominent conditions in first awards 1920-21, but organic heart disease showed considerable latency.
The functional condition Disordered Action of the Heart (DAH) was the third most frequently pensioned condition in the study (5.6% of pensioners) and the organic condition Valvular Disease of the Heart (VDH) the fifth (4.5%). In their PIN26 study (southern region) of WW1 pensions Jones et al found DAH made up 5.0% of pensions as a sole diagnosis and 6.9% as part of a multiple diagnosis. VDH made up 1.3% of pensions as a sole diagnosis and 1.6% as part of a multiple diagnosis.[84] Why the PLS should find a higher level in respect of VDH is not obvious.
Disordered action of the heart (DAH) - overview
The focus on heart symptoms in soldiers began during the Crimean campaign and the American Civil War. The problem was to explain heart disorders for which no organic explanation could be found, i.e. functional disorders (in modern terms, a software problem rather that a hardware problem). ‘Disordered action of the heart was a major cause of invalidity during the South African campaign of 1899-1902’,[85] at which time it was thought to be related to marching or tight packs, particularly in the case of those coming from industrial centres, ill-nourished and undersized.
The primary symptoms of DAH were breathlessness, pain, exhaustion, giddiness, and fainting. Exertion (DAH had also come to be called ‘effort syndrome’) came to be viewed over time as less related to carrying heavy kit or marching, and more to do with the general exigencies of war. Two specialised hospitals were set up to investigate DAH during WW1, under Thomas Lewis. Lewis ruled out heart valve problems but noted various blood/urine anomalies (although these specific factors faded in importance in further research). Lewis finally concluded that ‘it is conceivable that the symptoms arise … by the products of faulty metabolism engendered by infectious disease’. ‘Toxins, nerves, and overexertion’, in the final analysis, were seen as acting together.[86]
Other physicians would take the view that psychological factors in DAH were particularly important, and that it was ‘a manifestation of emotional disturbance and not the result of infection’ and that once a soldier had been given a diagnosis of heart disease ‘his fear maintain the symptoms and the symptoms maintain his fears’.[87] Oppenheimer and Rothschild at Colchester in 1918[88], looked at 100 cases of ‘irritable heart’ and found 61 with ‘a positive family or personal history for psychoneurotic factors’ and of these, 46 had a history of both. This group showed shorter service. Those without such history complained of chest pain, those in the ‘both’ group complained rather of ‘exhaustion and weakness’.
J A Venning reported two years worth of cases from No. 1 Convalescent Depot, and concluded DAH was ‘not a clinical entity, and the factors which go to produce the symptoms are numerous’.[89] He concluded that ‘undoubtedly the greatest factor in the production of symptoms of DAH is the physical and mental strain of war … it was impossible in many cases to distinguish whether the strain was chiefly mental or physical, the symptoms produced being identical’. He continued: ‘Infections come easily second as a cause’ (between 20 and 22%) ‘and by far the greater number of these were due to infections in civil life and not to PUO as has been widely held’. In terms of infections, rheumatic fever made up 41% of cases, Pyrexia of Unknown Origin 23%, with pneumonia next at 8%. ‘Nervous breakdown’ (including cases of such in civil life) accounted for between 6.4% to 10.3% (the variation depending on when during service the DAH manifested itself). 9.6% to 12.2% of cases were physically underdeveloped. Gassing was also deemed a factor.
Jones and Wessely note that ‘symptoms relating to the heart (palpitation, chest pain and shortness of breath) are prominent in both the debility and somatic clusters, which relate to disorders of the late nineteenth and early twentieth century’. It was the Second World War that would change views on ‘effort syndrome’. Research at Mill Hill Hospital by Paul Wood demonstrated a link between functional cardiac symptoms and ‘heightened emotional response to stressful activity’.[90] Jones and Wessely note, however, that Maxwell Jones, Wood’s collaborator, stated after the war: ‘There is no reason to assume that the condition has become less common—it is simply that the diagnosis E.S. is out of favour; psychiatrists in this country prefer to classify patients according to their psychiatric disability rather than their effort intolerance’.[91]
DAH in the pension ledger study
In the PLS there were 1,402 cases of DAH, and 140 cases of other ‘functional’ heart conditions, such as palpitations. These made up 6% of pension claimants. These individuals were those, clearly, who were protracted cases of DAH (many men during the war responded to rest followed by graded exercise).In the pre-war period (1854-1913) DAH in the military made up 2.1% of pensions as a sole diagnosis and 3.2% as part of a multiple diagnosis.[92]
The pension ledgers allow us to see what other protracted conditions were associated with DAH, set out in Table 27.

Table 27: Co-morbid diagnoses associated with DAH
Thus, only 60% of cases of DAH were sole diagnoses, and of the five principal associated conditions, medical conditions (including) infections and wounds (gunshot and gassing) comprised 33%. In contrast with the research done during the war, infections, psychological conditions and (particularly) gassing do not figure that highly in persistent and pensionable cases of DAH. Whilst there were 75 cases of a psychological condition (neurasthenia or shell shock) associated with DAH, there were only four cases of a psychological condition combined with a GSW being associated with DAH, and two cases of a psychological condition combining with a medical condition. The contribution of psychological conditions was therefore direct, and not mediated by medical conditions or wounds.
Paul Wood in 1941 concluded that ‘the division into sub-types of effort syndrome (constitutional, induced, psychoneurotic and physically fatigued) was ‘misleading if not meaningless’). He argued that effort syndrome was ‘an emotional reactive pattern particular to psychopathic personalities and the subjects of almost any form of psychoneurosis’.[93]
In a series of 50 cases where DAH was the only listed condition, the average percentage disability was 22%, ranging from 60% to 0%. Ten were rated as 30% disabled, and 16 as 20%. The highest rated, Private (316280) John Graham Brackenridge was actually initially rated 100% disabled, falling to 60%Pensiod at 24/- per week), both assessments (curiously) made in October 1919, his DAH ‘attributable’ to service. Lance-Corporal (493317) Wilfred Benyon, Labour Corps, was discharged in April 1918, aged 19. He was one of those individuals initially diagnosed with VDH, and a year after discharge was rated as 70% disabled (attributable). When exactly the change in diagnosis was made to DAH (aggravated) is not known, but in November 1920 he was rated 60% disabled, and a year after that 40% disabled. His final disability rating was 20% (8/- per week). Another young man, Private (TR3/72486) Arthur Stanley Butler was discharged in January 1919 aged 21. He was diagnosed with tachycardia (fast heart rhythm) and DAH, both attributable. Rated 20% disabled in March 1920, he was finally viewed as 14% disabled (7/6d per week).
The following case, although deemed ‘constitutional’ and ‘aggravated’, sets of the pattern of symptoms:
- Gunner (128935) Clifford Darwin, Royal Garrison Artillery, was discharged in April 1918, aged 40. His pre-war occupation was as a wooden packing case maker/dealer, and he had enlisted in December 1915. ‘A steady and hardworking man’, his degree of disability was finally rated as nil, and his board at discharge viewed his DAH as ‘constitutional’ (and representing 0% disability from the start). Symptoms became evident in May 1916, and he never served overseas because of his condition. His case was classic. In July 1917 his heartbeat was irregular and his pulse 135 beats per minute. In March 1918, ‘the heart beats are much increased by any exertion. The apex beat’ (the palpable cardiac impulse farthest away from the sternum and farthest down on the chest wall) ‘is displaced downwards. There is amount of arteriosclerosis. There is no muscular lesion’. Nine months later it was noted ‘at rest no murmurs after exercise’. However he was now rated as ‘less than 20%’ disabled with ‘irritable heart’. Fourteen months later in February 1920 he was described as ‘short of breath. Cannot stand fatigue’, but his DAH was regarded as ‘much improved, now negligible’, his heart sounds being improved. In September that year there was ‘slight arteriosclerosis, nothing else to note’. In October 1920 ‘no grounds for appeal’ was recorded. Whether he ever returned to his trade or not is not known – in 1939 he was a coffee shop keeper at the age of 60, dying at 72.
In the series of 50, five were cases originally diagnosed as VDH and changed to DAH. On such is:
- Alfred James Chaffey attested in August 1914, a 24 year old labourer who had served as a Volunteer in the Royal Garrison Artillery and was in the National Reserve, as Gunner (864) RGA. He was discharged on 18 November (‘character good’) with VDH. Despite this supposed affliction, he was working as a road labourer in 1916, and was conscripted that June, discharged a second time as Private (146327), Labour Corps, on 20 March 1919. At this point he was diagnosed with DAH ‘attributable’, consistently rated as 20% disabled between February 1920 and March 1923 (pensioned at 9/6d per week). The fact that he was discharged so quickly with an organic heart condition likely reflects inadequate medical assessment in August 1914. The fact that he returned to heavy labouring despite this is interesting. Whilst the change in diagnosis is not surprising, the fact that his DAH was finally deemed ‘attributable’ to service, suggests poorly joined up records and a history that was not transparent.
The following case illustrates the appearance of DAH two years after gassing:
- Sapper (465970) Norman Davidson, Royal Engineers (Electrical), had enlisted in November 1915 with ‘nil defects or aliments’. His trade was ‘pioneer (2 years as carpenter)’. His pension records indicate that he was gassed in October 1918, rated 20% disabled – ‘fundus and media are normal in each eye. He states he is occasionally troubled with them’. In January 1920 the concern was still about his eyes – ‘some excess of lacrimation’. His heart was checked – ‘no murmurs’. However, 11 months later the picture had changed: ‘C/O pains in chest, shortness of breath’, as well as ‘watering of eyes’. He was described as in ‘moderate general condition’, and his heart sounds were normal. In May 1922 he was described as ‘can’t get breath, eyes water, losing weight’. What started as eye symptoms matured over 3.5 years to a more general range of physical symptoms and he was pensioned for DAH ‘aggravated’. Initially pensioned at 8/- a week, in February 1922 his case was signed off with a payment of £10.
Jones and Wessely class DAH as a ‘war syndrome’. However, in the pension ledgers, 28% of cases were described as ‘aggravated’ and 1% as ‘not attributable’. DAH was therefore a feature of civilian life, and not just a war-related condition. If the conclusion reached at the end of the war that ‘toxins, nerves, and overexertion’ all played a part in a heterogeneous condition, then there would be no reason not to accept that it arose on civilian life as well. The fact, however, that 71% of cases of DAH were viewed as sole attributable to war, confirms the major role of the exigencies of service.
Valvular disease of the heart (VDH) - overview
VDH affects the four valves that open and close to regulate the blood flowing into and out of the heart. Symptoms include shortness of breath, chest pain, fatigue, dizziness, fever, rapid weight gain or irregular heartbeat. Causation is various – congenital malformation or other heart disease, or alternatively infection resulting from endocarditis (from blood infection), or rheumatic heart disease. Currently, some 2.5% of the population lives with moderate to severe VDH, increasing with age (13% of 75 year-olds). In terms of infection-related causation, rheumatic fever was a big killer in the years before the Great War, even in industrial societies – it would result from scarlet fever or strep throat, the latter now much better controlled with antibiotics.
Venning noted large errors in the diagnosis of heart problems during the war – 835 were admitted to the convalescent depot as organic, but the total was actually 304. Alternatively, of 304 cases admitted as VDH, 122 had been wrongly diagnosed as DAH. Venning also noted ‘a large number of the cases or organic lesions had stood many months of hardship and strain in the front line’.
VDH in the pension ledger study
In the PLS there were 1,123 cases of VDH, and 426 cases of other ‘organic’ heart conditions. These made up 6% of pension claimants. The average age of those diagnosed with VDH was 32. It was therefore not a condition of old men. It is likely that childhood illness in an era with inadequate medical care and no antibiotics comprised a significant number of these cases. Bland & Jones followed 1,000 children from 1928 with rheumatic fever, two-thirds demonstrating heart disease.[94] Half died over 20 years, 80% accounted for by rheumatic fever.
In the pre-war period (1854-1913) VDH made up 3.9% of military pensions as a sole diagnosis and 5.7% as part of a multiple diagnosis.[95]
In terms of the longer term, a study of 1,000 pensioned WW1 soldiers (rheumatic disease being known in half) showed that in the decade 30-40 years old, a third remined unchanged, a third progressed and a third died.[96]
Of the VDH cases indicated as the first condition, 48% were designated ‘aggravated’, and an exactly similar total of other organic heart conditions were also ‘aggravated’.
50 cases where VDH was the sole diagnosis, 25 ‘aggravated’ and 25 ‘attributable’ cases were randomly examined. The average disability in the ‘aggravated’ cases was 44%; and 39% in the ‘attributable’ cases.
An example of clearly worsening symptomatology (but not apparently related to childhood illness) is provided by the following case, which emphasises the Army’s preparedness to accept into service palpably sick men:
- Private (S/14880) William Victor Burn, finally 3rd Gordon Highlanders, was discharged on 7 April 1917, of ‘very good’ character, being ‘a very well-behaved soldier’. In December 1919 he was diagnosed with VDH of at least two if not three valves. The origin of his condition was dated to October 1915. He had joined the 16th Northumberland Fusiliers on 17 June 1915, at the age of 19 and a half years, and his symptoms emerged after about four months when he went for ‘a route march of about 14 miles. On the way back he fell down unconscious’. Two days later, ‘his sight suddenly became dim’. He was sent to the first Northern General Hospital. He remained there for two months, and was discharged from the Army two months later, returning to his work as a grocer. ‘His chums had all left and he could not stick it’, however, and he rejoined the Gordon Highlanders in June 1916. On his medical examination on rejoining it was noted: ‘Discharged as medically unfit about eight months ago. Mitral murmur of heart’. Accepted for service and undergoing further training ‘he reported sick once or twice on account of pains in the chest and breathlessness’, but despite this was remarkably sent to the Western front in September 1916. Two months later he ‘collapsed while at rifle drill’, and was hospitalised in the 24th General Hospital, Etaples, for a week and then invalided to the Northumberland War Hospital for a further six weeks. He returned to duty in January 1917. A week after his return ‘he dropped while drying dishes’. A range of heart symptoms were now identified. His record continues: ‘Rheumatism. Had growing pains when a child. Says he has never been ill in his life. Never had scarlet fever, diphtheria, rheumatic fever, nor St Vitus Dance. Not so caused’. When assessed before discharge it was noted: ‘Complains of pains over the region of the heart and breathlessness on exertion’. Neither his pulse nor blood pressure were abnormal. Although ‘polygraphic tracings show nothing abnormal’, a range of cardiac sounds were clearly abnormal, and his heart was enlarged. His condition was viewed as not attributable to service. Viewed as 50% disabled by ‘aggravated’ VDH, the rating was 80% disabled 10 months later, and 70% up to September 1922. Pensioned at 28/- per week, it is not known when William Burn died.
An example of significant impairment following childhood illness is provided by the following case.
- Sapper (308128) James Joseph Cowley, Royal Engineers, was 28 when he was discharged in February 1919, finally rated 70 percent disabled with ‘aggravated’ VDH (originally recorded as ‘due to’ service). His condition, ‘aortic incompetence’, was dated to ‘before enlistment’. It was noted that he ‘had scarlet fever at seven years, operation for hernia at 15 years’. ‘Hard work until enlistment and found no difficulty. First noticed shortness of breath etc. in November 1918 after a good deal of extra work’. (He enlisted in October 1915, and went to the Western front in May 1917). Hospitalised on three occasions, his symptoms involved ‘shortness of breath, palpitations, giddiness, pain in the chest’, and he demonstrated cardiac enlargement with abnormal heart sounds, although it was noted ‘exercise tolerance fair’. He was initially rated as 50 percent disabled and clearly deteriorated, and he was pensioned with 28/- per week. In civilian life he had been a fitter on the railways, and was still working in this capacity in 1929, despite his disability.
Another case indicates the difficulty in distinguishing between ‘aggravated’ and ‘attributable’.
- Corporal (4986) John Gordon Ashton was nearly 16 when he enlisted in the Lancers in 1905, having previously been a musician. He was transferred to the Reserve in 1912. Re-enlisting in 1915, he was discharged in September 1916, initially with haemorrhoids but whilst in hospital he was ‘troubled with cardiac pain and shortness of breath’. With VDH initially described as ‘aggravated’ and later as ‘attributable’, he was first rated as 50 percent disabled, and later as 20 percent disabled (pensioned at 8/- per week). With heart abnormalities and ‘dyspnoea on exertion’, he reported palpitations during 1917, when heart murmurs were detected. By 1920 he was complaining of shortness of breath and pain around his heart. A month before his death he was ‘admitted for VDH’, but was coughing up blood. He died on 25 February 1921, of aneurysm of the aorta and broncho-pneumonia. In the re-designation as ‘attributable’, it was presumably the matter of exertion during service that was key.
Rheumatism/arthritis/synovitis and myalgia
Of the skeletal and soft tissue conditions, rheumatism was the fourth most frequently pensioned condition, comprising 5.6% of claimants in the PLS, and myalgia the eighth (2.7%). It was a condition that demonstrated little latency. In the pre-war period (1854-1913) rheumatism made up 2.5% of military pensions as a sole diagnosis and 4.3% as part of a multiple diagnosis.[97] In their PIN26 study (southern region) of WW1 pensions Jones et al found rheumatism made up 2.6% of pensions as a sole diagnosis and 3.5% as part of a multiple diagnosis.[98]
Jones & Wessely[99] note that in the Boer War DAH and rheumatism were the primary ‘war syndromes’, the latter comprising ‘muscle and joint pain associated with fatigue … in the absence of organic signs such as inflammation and joint swelling’. Cold and wet (and infection) was assumed to be the causation. Rheumatism came under what they describe as ‘debility syndrome’. They noted that veterans ‘who had been awarded a pension for rheumatism showed no objective signs of the disease within a few years of discharge’.
In the PLS, 1,400 cases of rheumatism (5.5% of claimants) were recorded, and 268 cases of arthritis (1% of claimants). A diagnosis of the latter condition would have required more positive medical signs. Where rheumatism was the first recorded condition, 38% were noted to be ‘aggravated’, and 5% ‘non-attributable’ to service. Where arthritis was the first noted condition, 45% were recorded as ‘aggravated’ and 5% ‘non-attributable’.
Rheumatism
In a random sample of 50 servicemen with a sole diagnosis of rheumatism, the average final disability rating was 18%. The highest was 40%, and only six ratings were above 20%.
The following case gives an insight into the problem of diagnosing possibly vague symptomatology:
- Private (279589) Henry Batten, Labour Corps, was 52 in 1914. He had originally enlisted as Private (204571) in the Rifle Brigade. His transfer to the Labour Corps was undoubtedly on health grounds, and he was discharged on 9 October 1917 with a Silver War Badge. He was first diagnosed with debility and arthritis, the first ‘attributable’, the second ‘aggravated’. In October 1919 he was rated as 50% disabled. The first two diagnoses were retracted and replaced by rheumatism, first viewed as ‘due to’, and later changed to ‘aggravated’. Two months after his classification as 50% disabled he was rated as 10% disabled, a percentage remaining steady thereafter. His final pension was 5/6d with 1/4d in respect of his lone child, and in April 1921 his case was settled with a lump sum.
Synovitis
Synovial joints, such as the hip and knee, have a sheath of tissue known as a joint capsule that contains a synovium. This membrane produces a special fluid to lubricate the joint and prevent wear on cartilage while the joint is in motion. Injuries, osteoarthritis and various types of inflammatory arthritis can cause swelling of the synovium, which can lead to pain and other symptoms. Overuse is a cause but there is also a known link to arthritis.
191 cases of synovitis were noted amongst pension claimants, 84% being deemed ‘attributable’ to service.
Myalgia
Myalgia describes muscle aches and pain, which can involve ligaments, tendons and fascia, the soft tissues that connect muscles, bones and organs. Injuries, trauma, overuse, tension, and illnesses can all bring about myalgia. Differential diagnosis between this and rheumatism may not have been easy.
686 cases were noted amongst pension claimants, 63% of which were deemed attributable to service.
The average final disability in a group of 50 pensioners with myalgia as their sole disability was 17%, with a range from 0% (3 cases) to 80%. Only six individuals were rated as over 20% disabled, however.
A number of the pension claimants were older men:
- Private (40153) John Caulfield, Royal Defence Corps gave his date of birth as 1851 (verifiable in the 1911 census when he lived in Bangor, a general labourer). He enlisted on 21 April 1915, and was discharged on 1 January 1918, when he was 67. His myalgia was first viewed as attributable to service but then aggravated by, rated 40% disabled in September 1919 and 20% exactly 3 years later, when he was 71. He enjoyed his 8/- per week pension for a further three years, dying in 1925.
Tuberculosis
Pulmonary tuberculosis was the sixth most frequently pensioned condition in the PLS (4.4% of all claimants). It was a condition that demonstrated considerable latency.
Overview
In the 19th century TB, the ‘White Plague’ was epidemic in Western Europe, killing about a quarter of the adult population. Between 1851 and 1910 about 4,000,000 people died from TB in England and Wales – more than a third of those age 15 to 34 and half of those aged 20 to 24 died from the condition. By the end of the century 70-90% of urban populations were infected, many obviously with inactive conditions, and about 80 percent of those who developed active TB died from it.
Towards the end of the 19th century, however, death rates were declining, although the disease still remained one of the UK’s most urgent health problems at the start of the 20th century. Although the BCG vaccine was first used on humans in 1921 it would not be until after WW2 that it gained widespread acceptance in the UK. Thus, at the time of the First World War, containment was the only measure. There were campaigns to stop spitting in public places, and those with significant infection were pressured to enter sanatoria, with the supposed benefits of fresh air. Even under the best conditions, data from 1916 suggests that 50 percent of those who entered sanatoria were dead within five years.
TB most commonly involves the lungs (90 percent of cases), but in 15 to 20 percent of active cases it spreads outside the lungs causing other kinds of TB, particularly in those with weakened immune systems. General signs and symptoms of TB include fever, chills, night sweats, loss of appetite, weight loss and fatigue. The disease is transmitted (by those with active TB) by cough, sneeze, spitting, singing or even speaking when individuals expel infectious aerosol droplets. Poor ventilation and overcrowding in homes, workplaces and communities increased the spread of the disease; and poverty, malnutrition and hunger likely increased susceptibility to infection and severity of outcome.
The Official History(diseases) appears to play down the matter of TB. ‘There was in certain areas an increase in the peace-time ratios, but this increase is negligible from a wastage point of view in a world war’.[100] In terms of the ‘certain areas’, and in relation to the major theatres, the ratio of admissions per 1,000 troops for pulmonary TB was highest in Gallipoli (3.71); followed by the Western Front in 1915 (2.61); and Salonika in 1917 (2.14).[101] From the point of view of general public health, however, the OH refers to ‘latent development’ of TB in troops ‘worn out by war, disease, disease and service conditions’ who then returned to ‘overcrowded surroundings’ where TB was easily transmissible. ‘The wastage from this disease is negligible during war, the pensions burden to the State on its account after war is high’.[102]
It has to be observed, however, that Public Health England’s statistics show 80,788 ‘respiratory’ TB notifications in 1913, and 71,631 in 1918. The figure for 1919 was 61,154, and over the next decade showed a steady decline (with the exception of 1925) to 52,634 in 1929. There is no evidence that the return of infected servicemen led to any increase in pulmonary TB infections.
Pulmonary TB in the pension ledger study
In the PLS, 1,106 cases of pulmonary TB were recorded in in the sample of 25,000 servicemen, an incidence of 4.4%. The OH (statistics) considers pulmonary TB separately from respiratory conditions – if it were to be included as such in the pension ledger sample, the condition would comprise 32% of all lung conditions.
The incidence of pulmonary TB for the Army is 3.7%, that for the Navy 9.2%, and 6.2% for the RAF. The difference between the Army and RAF is likely related to the fact that the RAF comprised ground staff with many transferred from the Army on health grounds. The difference between the Army and Navy becomes more marked when those who served with the Royal Naval Division are considered separately. These men had an incidence of 5.8%. When these whose service was purely naval are taken the incidence was 11.7%, a rate three times higher than the Army.
The Navy did not keep records of TB during the war. In 1941 Surgeon Rear-Admiral S F Dudley observed that in the period 1900-1913 the invaliding rate from the Navy was 2.2% per thousand (any TB case was automatically invalided). ‘This critical morbidity of 2 per thousand is double that prevailing in the Army and Air Force’ and ‘the naval rate is considerably higher than that in men of the corresponding age and social class ashore’. The key factors, Dudley gave opinion, were ‘air space’ and ‘closeness of community life’ for ratings (officers having half the rate of incidence).
The PLS would suggest a five-fold increase of pulmonary TB during the war in the Navy. Given that over-crowding and proximity were viewed as keys factors, the question arises as to why would crowded billets not produce a similar effect for the Army? The answer may lie in better ventilation.
According to the Official History (statistics), TB made up 8.8% of ‘conspicuous disabilities’ in First Awards.[103] The disease comprised 11,032 (2%) of 572,125 of stabilised award cases to 1929, and 20.7% of 113,207 unstabilised pensions to 1929.[104] Given that the pension ledger sample is comparable to the army as a whole, with the addition of the Navy and RAF, the total cases which would be predicted from the sample of 685,332 cases (Stabilised and Unstabilised) would be in the region of 30,400, slightly less than the actual figure of just over 34,000. The discrepancy may lie in the fact that the 34,000 figure includes all types of TB (see below).
In a random sample of 50 servicemen pensioned for TB of the lung alone (six of whom were noted subsequently to have died), the average disability was high, 70%. Nineteen men (38%) were rated at 100% disability, and 60% were rated 70-100% disabled. The Official History (statistics) gives 35.2% of unstabilised awards as 70-100% disabled, and 45.3% of stabilised awards.
Thirty-four per-cent of ‘first-listed’ cases of pulmonary TB in the ledgers were described as ‘aggravated’ (as well as four per cent as ‘not attributable’). This means that 62% of cases were regarded as arising anew during the war. Given that a sputum test is the only way of confirming a TB infection, it must be concluded that in the ‘aggravated’ cases a cursory medical examination would have had little chance of picking up a man with no obvious symptoms. Yet these individuals would have been the disease spreaders infecting the remaining 62%.
From the 50 individuals three sets of extant pension records provide two cases of ‘aggravated’ pulmonary TB, and one ‘attributable case’.

Above: Military TB cases in a sanatorium sun parlour (Library of Congress/2002646775)
The following two cases outline ‘aggravated ‘ pulmonary TB, the second demonstrating the inadequacy of medical examination in the first six months of the war:
- Lance-Corporal (3621) John Burns Findlay had enlisted in the Scottish Horse in 1910, his job being on the Caledonian Railway. He served on the Western Front from August 1915 to February 1916. In September 1919 he was rated 100% disabled by pulmonary TB, which was described as ‘aggravated’. His medical examination in 1910 reported good chest expansion and his physical development as ‘very good’. He would not have been medically examined in 1914 when, perhaps, evidence of his TB might have been more evident. He died in 1922 at the age of 38.
- Bernard Gillies, a labourer in civilian life who was aged 36 on the outbreak of war, served both as a Gunner in the Royal Garrison Artillery (6055) and as a Private in the Royal Scots (26357). He was discharged first from the artillery in July 1915 (having attested that January), medically unfit, and from the infantry in November 1915, having served 113 days, ‘not likely to become an efficient soldier’. In 1919 he was viewed as 100% disabled with pulmonary TB, described as ‘aggravated’. His wife Catherine had died in February 1915 of pulmonary TB, whilst he was at the regimental depot at Great Yarmouth. His (second) discharge from the Royal Scots was on account of his TB, and it was noted that he had had treatment in a Dundee sanatorium in autumn 1914. His medical examination in July that year, at his second attestation, a mere 14 days after his discharge, rated his physical condition as ‘good’.
Gillies’s case demonstrates three things. Firstly, the likely transmission of the disease within a household, although we do not know whether husband infected wife or vice versa. Secondly, it may seem extraordinary that a man with a history of sanatorium treatment for TB four months previously could be passed medically fit for service, and then, having been discharged, be taken on by the army again immediately, lasting only 113 days before being discharged with the condition active. It suggests medical examination with no relevant history taking. Thirdly, the fact that on his second discharge his TB was not seen as attributable to or aggravated by military service, yet in 1919 the ‘not attributable’ statement is crossed out and ‘aggravated’ substituted suggests a certain generosity on the part of the examining doctor.
A third case gives an example of a condition apparently acquired during the war:
- Private (15093) George Henry Harris, a gardener, had joined the RAMC in 1901, aged 18, ‘fit’ and ‘will probably develop to standard’. He saw service in South Africa in 1901 and on St Helena. He was re-engaged after his first term of service expired, and served on the Western Front from August to November 1914, and on Gallipoli to August 1915. At this point he returned to the UK to be discharged ‘no longer physically fit for war service’ a year later. In 1919 he was rated 80% disabled with ‘tubercle of lung’, ‘attributable’ to war service. He would not have been medically examined in 1914, and assuming a developing TB would have picked up in service before then, and presuming an adequate medical history was taken for pension assessment purposes, his illness was acquired during his three months on the Western Front or four months on Gallipoli.
Other TB in the pension ledger study
112 cases of TB other than pulmonary were recorded in the pension ledger sample. This represents nine per cent of all TB cases, somewhat less of the 15-20% that might be overall expected, which may represent something specific to service conditions rendering individuals more vulnerable to pulmonary TB; or may simply be a reflection of latency in spread.
Table 28 lists the nature of these conditions in terms of location in the body, the lymph glands of the neck and the testicles being the top two infection sites.
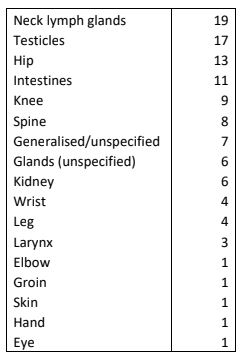
Table 28.TB cases other than pulmonary
Debility
Debility, as a sole diagnosis, was the seventh most frequently pensioned condition in the PLS(2.8% of claimants). In the pre-war period (1854-1913) debility made up 1.4% of pensions as a sole diagnosis and 6.2% as part of a multiple diagnosis.[105] In their PIN26 study (southern region) of WW1 pensions, Jones et al found debility made up 2.5% of pensions as a sole diagnosis and 4.4% as part of a multiple diagnosis.[106] None of the volumes of the Official History (medical) deal with debility as a condition.
Debility is, of course, a symptom rather than a condition in its own right. Its modern definition is ‘a state of general weakness or feebleness that may be a result or an outcome of one or more medical conditions that produce symptoms such as pain, fatigue, cachexia and physical disability, or deficits in attention, concentration, memory, development and/or learning’. There are, of course, modern correlates in ‘chronic fatigue syndrome’ (CFS) and ‘myalgic encephalomyelitis’ (ME), but we cannot assume that these are necessarily identical to the concept of ‘debility’ 100 years ago. CFS and ME may be genetically determined, or related to viral/bacterial infections, problems with the immune system or hormone imbalance.
Debility, in terms of its Great War usage is connected with a range of conditions. The phrase ‘nervous debility’ is also used, however. It is interesting that a note from 36 Casualty Clearing Station (30/11/1916) states: ‘’The institution of 21 CCS as a sorting place for shell shock etc. is having a marked effect – but the diagnosis is so often changed to Debility, i.e. a case who would, a month ago, be sent to a Field Amb(ulance) as shell shock or neurasthenia is now sent as ‘”exhaustion” & some trivial & insufficient ailment’.[107] In the PLS, ‘nervous debility’ is classified and analysed as psychological condition.
Debility in the pension ledger study
697 claimants were pensioned with a sole diagnosis of debility. Interestingly in 98% of cases this was listed as the first condition, and of these, 34% were regarded as ‘aggravated’ or ‘non-attributable’.
However, when debility is listed with another condition, it rises to include6.4% of all pension claimants.
Sole condition 43%
Infection 30%
Other medical condition 15%
DAH 2%
GSW 2%
Gassed 1%
Nervous debility 7%
It cannot, of course be guaranteed that when debility is listed as a sole condition, it did not originate in an infection or other medical condition now resolved, but these figures indicate that in nearly 5 out of 10 cases, debility was linked to such. It is interesting that GSWs and gassing resulted in very few separate diagnoses of debility.
The average disability rating was 19%. Eleven ratings were over 20%, one at 50%, but five were also rated zero disability, even though the condition was viewed as either attributable or aggravated.
There was a recognised connection between debility and age.
- Sapper (196158) William Duncan, Royal Engineers, was a 51 year-old wool-spinner from Carlisle in 1914. He served overseas and was pensioned in December 1917, when he was now 55, ‘over age and debility’, deemed ‘aggravated’. In January 1920, he was judged 50% disabled, then 40%, dropping to 30% three years later.
- Private (426549) Robert Duncan, who was 50 in 1914, began the war in the Royal Garrison Artillery, transferred to the Labour Corps (presumably on health grounds). Discharged in September 1918, and rated as 5% disabled in August 1919, his conditions were given firstly as ‘age’ (charmingly described as ‘aggravated’), and debility (also ‘aggravated’).
An awful case of multiple conditions is illustrated by the following serviceman, of whom it must be questioned as the whether he was sufficiently compensated:
- Private (130170) Samuel John Chaney (a colliery haulier)enlisted on 19 August 1914, and was discharged on 6 March 1919. Aged 26 in August 1914, he served first in the South Wales Borderers (12521), going to the Western Front in June 1915, and then in the Labour Corps (54 HSE Company). His pension ledger record lists his first condition as ‘debility following dysentery’ There then follows in brackets; ‘GSW head, rheumatism, bronchitis, malaria’ (the rheumatism carefully marked as ‘due to nil’). In August 1919 he was viewed as 40% disabled, a year later as 30%, and in August 1921 as 6-14% disabled (and pensioned at 13/6d. In 1939 he was working as a labourer in a steel works despite his health record.
Kidney and other urinary tract conditions
558 pensioners were diagnosed with kidney-urinary tract symptoms, 2% of total pensioners in the PLS. As will be seen from Table 29, the bulk of these were cases of nephritis, with other urinary tract infections such as cystitis, given here for comparison, relatively small. Other kidney/urinary tract conditions included haematuria (not diagnosed as related to any condition); stricture of the urethra (likely indicative of a prostate problem); urinary incontinence; kidney stones etc).
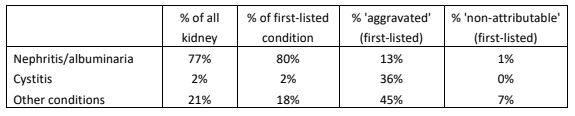
Table 29:Kidney & urinary tract conditions in the PLS
Overview
Nephritis (known also as Bright’s Disease, and associated albuminaria) is the only kidney/urinary tract condition that the Official History (diseases) considers.[108] It is a range of conditions in which the nephrons, the functional units of the kidneys, become inflamed. Albuminaria, the presence of protein in the urine, was generally taken as indicative of the inflammatory lesions of the kidney associated with nephritis. Causation is of many different types and such may never be clear.
‘Trench nephritis’ began to be recorded in the Army on the Western Front from February 1915. In following years cases were more pronounced in the winter months, and were often viewed as complications of primary respiratory disease. In some men there was a chronic kidney condition, made symptomatic by current infection. The majority, however, were free from renal disease at the moment of onset.[109]
There were two types, one involving pyrexia and blood in the urine; the other characterised by ‘dropsy’, oedema in modern parlance, i.e. water retention in tissue, the legs in particular (this second type being the larger group). Shortness of breath might be observed, as might headache and palpitations. Age was not a factor. Mortality was very low.
Nephritis in the pension ledger study
Nephritis made up 1.7% of pension claims. Of those where the condition was first listed, in only 13% of cases was nephritis considered as aggravated by or not attributable to service The average level of disability in a sample of 50 men for whom nephritis was the sole pensionable condition, was 30%. The range was 100% to zero, although only six disability ratings were over 50%.
The following case gives an account of the course of the condition and investigations:
- Private (50918) Ernest James Harvey, Manchester Regiment, was rated as 6-14% disabled with nephritis at the age of 40 in 1922 (pension of 11/6d per week). ‘A steady & well behaved man’, of ‘good’ physical development on attestation (albeit with defective teeth and some eczema), his discharge documents of September 1918 show he had suffered a GSW wrist a year earlier, at which time he had been noted to be suffering cystitis. The nephritis (he was not pensioned for the GSW) was dated to the time of his diagnosis with cystitis, and initially he was deemed 70% disabled on discharge: ‘Urine has consistently contained 25% albumen, occasional blood, headache’. Disability decreased to 50% then to 30% by May 1919, at which point it was recorded: ‘No oedema of feet, urine no alb(umen)’. This was the same picture in February 1920, but Harvey was complaining of ‘giddiness, gets easily tired’. Thirteen months later, his blood screening was mostly normal, although his tongue was ‘furred’ (this could have many causes) and his teeth ‘defective’ still, and rated 20% disabled. A pre-war water tester, in 1939 he was working as a house painter, an indication that the wrist injury had proved no lasting issue.
The following case involves a complex individual:
- Private (2913) John Gannon was a 21 (or 23) year-old labourer of ‘good’ physical development, who enlisted in the Coldstream Guards in 1899. Transferred to the Reserve in 1902, he was re-engaged in 1911. Clearly a difficult man, he had a string of ‘offences’ which continued throughout the war, including drunkenness, being AWOL, and insubordination, and ‘emptying his water bottle’ In July 1915, however, he was diagnosed with nephritis (and also with gonorrhoea that December, a condition which he appeared also to have been treated for in 1901, and which would have been unconnected), and was sent to hospital in the UK. In 1918 he was also diagnosed with rheumatism and myalgia, and was evacuated to the UK the day before the Armistice. Despite these various conditions, his pension was based only for his nephritis, deemed attributable to service, and he was rated 20% disabled in 1920, and 14% in 1922 (pension of 8/6d per week).It is interesting that a man with such a difficult relationship with authority was only pensioned for one out of three conditions that arose during the war. It is also interesting that given his convictions for drunkenness, and the strong prevailing belief that alcoholism and nephritis were linked, that his condition was deemed attributable to service. Gannon died in 1946 of cerebral thrombosis and arteriosclerosis.
Two cases – ‘attributable’ and ‘aggravated’
- Gunner (94583) Edgar John Evans, Royal Garrison Artillery (262 Siege Battery), was 30 when he attested at the end of 1915, his trade being that of tailor. After nine months on active service he was invalided to the UK and admitted to Oakbank War Hospital Glasgow in July 1917 and discharged in July 1918. His nephritis was viewed as ‘attributable’ to service, but his degree of disability was rated as ‘less than 20%’ and he was awarded 5/6d a week, his wife 3/6d, and his child 1/4d. In 1939 he was still pursuing his job as a ‘tailor’s fitter and passer’.
- Private (4551) Joseph Bell, Royal Lancaster Regiment, demonstrated the fluctuating nature of nephritis. He was 38 at the outbreak of war, and his condition was described as ‘aggravated’. He was discharged in June 1916, and there is no evidence that he served overseas. In 1920 he was rated as 50% disabled, the same a year later. Twelve months on again, in 1922, he was now rated as 100%, the same rating given six months later. Confusingly, a reassessment three weeks later gave a 50% disability rating, the same being given three months later in 1923, with two undated ratings of 100% and 50% (pensioned at 20/- per week, 10/6d for his wife).
Other trench conditions
Infections
In terms of other trench or demonstrably service-related conditions, with respect to infections, amongst pension claimants there were:
Trench fever 110 cases
Pyrexia of unknown origin (PUO) 13 cases
Trench fever was marked by febrile periods with headache, local pain, rash, and spleen enlargement. The rate of incidence of these infections is not exactly clear – from July 1917 to June 1918, in Second Army there were 15,392 PUO cases and 5,244 trench fever cases.[110]
It is now known that trench fever is a louse-borne disease caused by the bacterium Bartonella quintana, and whilst there were indications of this prior to the war, considerable research on cases to 1918 confirmed this. Whilst over 83% were discharged to duty within 60 days,[111] in cases invalided home (11.5% of those affected) there was ‘a tendency to advance through a subacute towards a chronic condition with symptoms of disordered action of the heart, and also in some cases of neurasthenia.’[112]
Evidently, if only 110 cases were granted pensions on the basis of trench fever alone, it might be thought that its effects were not unduly permanent (prolonged ill-health was noted in 10-20% of cases)[113]. However, according to the OH, pensions were granted for DAH in 19% of cases; debility (13% of cases); and myalgia (6%)[114]
Cases of PUO often turned out to be trench fever (66% in one study).[115] Clearly the infrequency of these two conditions appearing in the pension ledgers indicates the preference of other diagnoses.
Medical conditions related to adverse climate
In terms of conditions that were related to hostile environment, in the pension ledgers there were:
Trench foot 110 cases
Frost bite 61 cases
Heat stroke 17 cases
0f the 94 cases of amputation where GSWs are not mentioned, the majority are fingers. Some however involve trench foot and frost bite.
- Private (23546) Owen George Brown, Royal Welsh Fusiliers was discharged on 27 April 1916, 30% disabled, ‘partial amputation, frostbite, loss of 3 toes’.
- Private (3/10793) Thomas Herbert Oldham, Leicestershire Regiment, was discharged on 20 April 1916, 20% disabled, ‘frostbite of toes’, his big and 2nd toe of his right foot and the little toe of his left foot having been amputated.
- Private (17666) Arthur Davison, North Staffordshire Regiment, was discharged on 12 June 1916, 30% disabled, ‘trench feet, amputation both big toes’.
- Private (25691) Charles Genner, West Riding Regiment was discharged on 1 March 1919, aged 37 and 70% disabled, ‘amputation of all toes of both feet (trench feet)’. A similar outcome was reported for Private (6584) Patrick Wright, Royal Munster Fusiliers, rated 50% disabled.
- The pension ledger of Private (27318) George Henry Thacker, 18 in 1914 when he worked as a hairdresser, and discharged on 18 December 1917, states ‘trench feet, amp(utation) toes’, and he was rated 55% disabled. Thacker’s pension records survive and tell a more dramatic story. He had been wounded in the back by a shell on 22 October 1916, ‘Paralysis of R leg, lay in shell hole 3 days unable to move & without food. Gangrene of toes of both feet’. There was a vertebral fracture, a lesion of the spinal cord, and penetration of his abdomen’. He had been posted to the 1st Battalion Royal Lancaster Regiment only 30 days before his injury. His spinal injury recovered to the point of ‘anaesthesia of left sole’. Both his big toes had been amputated, ‘also smaller portions of other toes’. Clearly this was viewed as his major remaining injury. He returned to his job as a hairdresser (obviously requiring standing) which he was still pursuing in 1939.
Digestive system conditions
The Official History (diseases) informs us that ‘intestinal disorders … furnished a considerable proportion of casualties on all fronts; more especially was this the case in the tropical and subtropical theatres of war’.[116]
Of the seven major digestive system conditions examined by the PLS (see Table 30), only two were, however, deemed to warrants chapters in the OH, enteric fever and dysentery, the latter seen as a particular issue. (Cholera was given a chapter, but there are no cases in the pension ledgers).
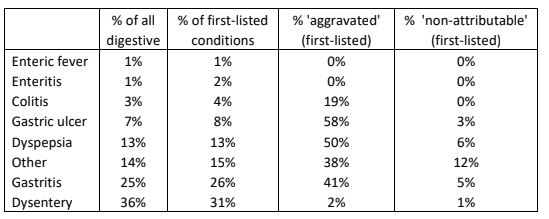
Table 30. Digestive system conditions in the pension ledgers
In the PLS:
- The smallest group recorded was the enteric group of fevers. This was a term used loosely by medical officers, covering both typhoid and paratyphoid fevers; the first (a bacteria, Salmonella typhi) producing both general and gastric symptoms, is related to poor sanitation and unclean water; the second (with two types), with similar symptoms, is caused by different Salmonella bacteria. The low levels seen in the pension ledgers reflects the lower levels seen in the Great War in comparison with the Second Boer War.
Enteritis, with more specific gastric symptoms, is the result of either viral or bacterial infection, leading to inflammation of the small intestine. Again, its incidence is low in the pension ledgers.
Notably, enteric fever and enteritis, although the number of cases is relatively low (12 and 18 respectively), all were considered as attributable to service.
- Colitis, representing 3% of all gastric conditions in the pension ledgers, is largely caused by infection, and chronic cases can develop into ulcerative colitis and Crohn’s disease. Again, gastric symptoms are prominent, with weight loss and fatigue. In contrast with enteric fever and enteritis, 13% were seen as ‘aggravated’.
- Gastric ulcers (stomach and duodenal) are almost all caused by H. pylori bacteria, with some people more vulnerable. In the PLS, 58% were seen as ‘aggravated’ and 3% ‘non-attributable’.
- Dyspepsia, of course, is a common problem, affecting 30% of the population currently. In modern medicine, the term for recurring indigestion that has no obvious cause is ‘functional dyspepsia’, with symptoms similar to an ulcer – pain/discomfort in the upper abdomen, often accompanied by bloating, belching and nausea. In the pension ledgers we are probably seeing cases of this longer term ‘functional dyspepsia, where 50% of cases were seen as ‘aggravated’ and 6% ‘non-attributable’.
- Gastritis, the second most common condition in the pension ledger gastric conditions, comprising a quarter of all such, isa group of conditions that involve inflammation of the stomach lining, most often the result of infection by the same bacteria that cause stomach ulcers. 41% of cases in the pension ledgers were seen as aggravated, with 5% ‘non-attributable’.
(Conditions listed under ‘other’ include poorly defined matters such as ‘stomach trouble’, ‘inflammation’ ‘dilation’, constipation, or ‘gastric catarrh’; and structural conditions of the alimentary tract such as abdominal adhesions, peritonitis, anal fistula, rectal prolapse, rectal abscess or polyps, sphincter paralysis, etc.)
A tentative conclusion might be drawn is that gastric conditions were far more frequent in the general population of 1914 than the population of 100 years later.
Dysentery in the pension ledger study
Dysentery is the second of the conditions deemed worthy of a chapter in the Official History (diseases). Three types of dysentery were noted, none specifically identified in the PLS, where they comprised over a third of cases of gastric symptoms, 97% deemed ‘attributable’ to service. As noted earlier, there was an overlap with malaria, co-morbid dysentery being noted in 4.4% of cases.
The average level of disability in a sample of 50 men for whom dysentery was the sole pensionable condition, was 20%. The range was 60% to 5%, although only two disability ratings were over 50%.
The following case gives an account of the course of the condition:
- Lance-Corporal (12370) Bob Lockett, Machine Gun Corps, was discharged in February 1919, aged 30. On 13 August 1914 he was rated as of ‘very good’ physical development, and he worked as a tailor. He served first in the 7th North Staffordshire, and landed on Gallipoli with them in July 1915. The unit then went on to Mesopotamia, but at some point Lockett transferred to the Machine Gun Corps. In September 1917 he was in hospital in Staffordshire for 35 days with accidental second degree burns to his right foot. His dysentery was dated to August 1915, shortly after his arrival on Gallipoli. In October 1919 he was rated 20% disabled. Medical examination noted: ‘Diarrhoea. No blood, bad slime.’ His last attack was six days before examination. ’18 lbs loss of weight since August 1914’. ‘Some dyspnoea’ (laboured breathing). ‘Tenderness across ascending colon’. In March 1920 it was noted: ‘C/O pain in r(ight) side below liver. Diarrhoea 5 weeks ago. Pain in r(ight) knee.’ His liver was tender, and their was dyspnoea and dizziness. There was also ‘tenderness over colon’. He was now rated as 40% disabled (having been rated 60% disabled a few weeks earlier, with a pension of 24/- per week). At his next examination (date not clear) he was ‘C/O diarrhoea, slimy motions, 3 this morning. Pains in stomach, pains in knees and shoulders’. There was ‘some dyspnoea & giddiness’, but he was now rated as 20% disabled once more. That September it was noted: ‘Stool no pus, blood found’. In January 1923, it was recorded ‘3 motions daily. No pus or blood now’, but his liver and colon were still tender. In March 1923 there were no findings of dysentery and he was rated as ‘nil disability’.
Another Gallipoli case demonstrates a higher disability rating and early discharge:
- Private (17799) William Henry Cook, Sherwood Foresters, was discharged in August 1917, at the age of 23, rated as 60% disabled with dysentery. He joined the Mediterranean Expeditionary Force on Gallipoli on 1 July 1915 and returned to the UK on 16 October, where he remained until discharge.
Two cases link dysentery and debility:
- Gunner (186225) Robert Davies, Royal Garrison Artillery, has two diagnoses in his pension ledger record: (i) Debility ‘due to 30%’; and (ii) Effects of dysentery ‘due to’, with the remark ‘change of diagnosis’ between the two entries, which could be taken to read that the debility was the ‘effects of dysentery’ referred to. In August 1919 he was rated as 20% disabled, and then in each of the next two years, at 5%. At the end of 1921 (a year in which he was examined twice) he was rated 20% disabled once more and the following year 6-14% disabled ‘declared final’, with a weekly pension of 12/6d.
- The pension ledger of Driver (193132) John Kidd, Royal Field Artillery, bears the diagnosis ‘general debility following dysentery’, and ‘due to’ service, but strangely he was rated as ‘nil’ disability and simply given a grant of £5.
Finally, a quite extraordinary case of dysentery with multiple conditions and two distinct pension claims:
- No British records of any sort, not even a medal card, apart from the pension ledger record, exist for Sapper (WR552508) Hubert Byrne, Royal Engineers, discharged in May 1919, and rated 15% disabled with dysentery, sand fly fever, and malaria, ‘attributable’ to service. Sandfly fever was endemic around the Mediterranean, but not as noxious as malaria. Byrne certainly had a mix of conditions, however.
His address is given as Donore Avenue, Dublin. Records exist, however, in the Irish Military Service Pensions Collection, for Hubert Byrne at the same address. Byrne was rated in these documents as 20% disabled, but for his IRA activities, claiming that his wounds were ‘keeping me from earning my living as well as I used to’ (he worked as a carpenter). He had sustained GSWs to both arms in July 1922 at the Hammam Hotel, O’Connell Street, Dublin, fighting against Free State Forces, when he was a member of the Criminal Investigation Department, an armed, plain-clothed counter-insurgency police. He was subsequently interned as an IRA prisoner, and there are suggestions he was providing intelligence to the ‘National Army’ at this time. In 1916 he was a member of ‘Liverpool circle’, Irish Republican Brotherhood, C Company, 4th Battalion, Dublin Brigade, and claimed to have been involved in fighting in Dublin that April. In 1916 he acknowledged that he had been ‘arrested as a conscript’ (he had returned to Liverpool, and whilst there was no conscription in Ireland he was understandably reluctant to connect himself so recently to Dublin), but (perhaps wisely) gave the Irish authorities no information about his service with the British Army. In fact, he described himself ‘not a good soldier’, and held ‘practically a prisoner until the war was over’, in ‘”civvy” clothes’. This was manifestly not true. He died in 1956, aged about 65.
Deafness
Deafness was the ninth most frequently cited pensionable condition (2.4%). 45% of cases were deemed aggravated or non-attributable. Of a sample of 50 servicemen with ‘deafness’ as their sole diagnosed condition, the average disability was 26%. Four were rated 50% or more disabled, 28 were rated 20% or below disabled.
Much of the hearing loss would have been caused by infection, notably otitis media. The extent of the role of the noise of shellfire is unclear. Repeated loud noise can cause a build-up of wax in the inner ear which may lead to infection. Alternatively, most noise-induced hearing loss is caused by damage to the hair cells in the inner ear which set up the electrical signals to the auditory nerve.
It is possible to contrast the number of pension claimants between those who dealt explosions (the artillery) and those where were on the receiving end (the infantry). The percentages are 3.7 in the artillery claimants, and 1.9 in the infantry. Whilst this might be suggestive, deafness in Royal Naval (i.e not RND) claimants who, it might be supposed, were much less frequently exposed to explosions during the war, comprised 1.4% of cases, not far behind the infantry.
Some cases were caused by long-term infections, many of which may have been pre-war:
- Private (52920) George William Doe, 8th Battalion Royal Fusiliers, was 21 when he was discharged in February 1918, with ‘deafness’ deemed ‘aggravated’ by service. (His records refer to an attack of bronchitis in July 1917 and ‘slight neurasthenia’, but these do not reappear in his pension ledger). Rated 40% disabled on discharge, in February 1920 he was deemed 20% disabled, 30% 15 months later, rising to 80% in April 1921 and finally 30% in December 1922 (12/- pension per week). A time keeper clerk, he had enlisted in April 1916 (having served with the 5th Durham Light Infantry, until October 1913, discharged due to bronchitis, apparently suffering repeated attacks of this infection ‘since birth’), and had gone to the Western Front in February 1917, his overseas service lasting five months. He informed that he had ‘had right ear trouble since he had measles in childhood’. He had undergone a mastoid operation, but this was followed by ‘continuous discharge’. He was totally deaf in this ear, and suffered ‘giddiness’. It may be wondered how these matters escaped medical examination.
Another case illustrates the possibility of noise setting up infection:
- Private (555244) William Cuthbert was 26 when he was discharged from the Labour Corps in July 1918, rated 30% disabled with ‘deafness’ deemed ‘aggravated’ by service. A coal miner in civilian life he had previously been in the Special Reserve of the Royal Field Artillery, and claimed that his ear problems had started on pre-war camp at Oakhampton. (He was treated for gonorrhoea in the pre-war period but this is not known to cause deafness). His problem was detected on mobilisation, and he was put on ‘light duty’, firstly in the RFA Officers’ Mess at Exeter, the anti-aircraft observation, and finally office work for the Labour Corps. The cause was seen as ‘gun-fire (pre-present war)’. Cuthbert himself claimed to have been firing an anti-aircraft gun. His left ear was inflamed, with suppuration, and otitis media was diagnosed.
Three cases within the 50 were specified as traumatic in origin:
- Private (265628) Harry Brewer, King’s Own Royal Lancaster Regiment, was 21 when he was discharged in March 1917, having served on the Western Front since May 1915. He was diagnosed with ‘traumatic perforation of membrane tympanorium with deafness’, and rated 20% disabled, ‘due to’ service. How this happened is not known.
- Private (54381) Owen Davies, Welsh Horse then 19thRoyal Welsh Fusiliers when he was 24 when he was discharged in May 1918. 80% disabled (pensioned at 20/- per week), the cause of his ‘complete deafness’ was ‘concussion of labyrinth’. This seems very likely to have resulted from shellburst.
- Private (3/3535) William Pace, Black Watch, was 30 when he was discharged in August 1915, 40% disabled with a diagnosis of ‘deafness (shell explosion)’. He received 16/- per week with 9/5d for his wife and child.
Defective teeth/vision
(i) Dentition
Dental health was very poor in the early 20th century – 70 per cent of British recruits were regarded as in need of dental treatment. In 1914 there were only 20 trained dentists in the military. The term ‘trench mouth’ was coined during the First World War, and describes an acute gum infection that involves painful necrotising ulcers throughout the mouth. No dental surgeons were sent to France in 1914, but by 1918, 800 were serving in the army either in the field or at home. The Official History notes that many men were rejected in 1914 on the grounds of the state of their teeth, when some dental treatment would have rendered them acceptable.
- Sixty pension claimants had ‘defective teeth’ as the first listed condition, 60% of these described as either ‘aggravated’ or ‘not attributable’ to service, and this condition typified 2.8% of claimants overall.
(ii) Eyesight
The eyesight standard in the British Army in 1914 was the lowest in the European armies – the standard required in the latter being 6/12 with/without glasses (meaning that one can see at a distance of 6 meters what a normal person can see at a distance of 12 meters), whereas it was 6/12 unaided in the British Army. For those who passed the test, King’s Regulations (1704) stated: ‘Glasses may be worn by all ranks on or off duty’.
- 204 pension claimants had ‘defective vision’ as the first listed condition, 69% of these described as either ‘aggravated’ or ‘not attributable’ to service, and this condition typified 1.4% of claimants overall.
That 69% should be deemed ‘aggravated’ or ‘not attributable’ seems to suggest shortcomings in the eyesight element of the medical exam. W H A Groom attempted to enlist in the London Regiment in March 1916, wearing glasses, and was told that ‘I must pass the battalion test, so upstairs I went where a corporal gave me an eye test which I failed by one line without glasses’. He immediately tried the Honourable Artillery Company where, again, ‘all was well except for the eye test’. Two weeks later he was summoned for a routine conscription medical examination at the White City, choosing not to wear glasses. The test card being left unattended, he memorised the failed line, and passed.[117]
Sexually transmitted diseases
Much has been written on the prevalence of STDs in the British, Australian and Canadian forces during the First World War. Although their occurrence in the pension records is small (57 cases), it is perhaps surprising that they are there at all.
General Paralysis of the Insane/Neurosyphilis
General Paralysis of the Insane (GPI), is a possible outcome of tertiary syphilis (the last stage of an untreated infection. Current estimates are that 15-30 per cent of untreated infections will proceed to what is now known as neurosyphilis). It is a terminal condition resulting from neurological degeneration.
Syphilis was a true plague of the Victorian era. The Royal Commission on Venereal Diseases reported in 1916 an overall prevalence in the population of 7.8 per cent, and gave opinion that the rate ‘cannot fall below 10 per cent of the whole population in the large cities’. Syphilis formed roughly a quarter of the 400,000 venereal infections in the British forces during the war; the Canadians estimating a prevalence of 4.5 per cent in their troops. It was a common but incurable disease of the age. Twenty per cent of male mental asylum admissions during this period were cases of GPI.
GPI emerges between 10 to 30 years after infection, and from diagnosis to death is a period of three to five miserable years. None of the 17 claimants for GPI therefore contracted syphilis during the war. There were 15 cases of Tabes Dorsalis (where there is syphilitic damage to the spinal cord and peripheral nervous tissue)and Cerebrospinal Syphilis.
(i) Neurosyphilis
Cases of GPI were rated 86% disabled on average; cases of Tabes Dorsalis/Cerebrospinal syphilis being rated 75% disabled.
There were no neurosyphilis claimants from the RAF. 1% of army claimants were such cases, whereas 6% of naval claimants were neurosyphilis claimants. In the naval cases, assessing doctors were far more ready to designate ‘not attributable’ rather than aggravated.
A case of GPI ‘aggravated’:
- Herbert Ashman first served as Driver (T2/10237) Army Service Corps (Meerut Divisional Train) – the qualifying date for his medals is 04/10/1914. He then served as Gunner (191538) Royal Garrison Artillery, and finally as Private (701503) in the Labour Corps. Aged 41 in 1914, he was discharged on 6 December 1919, and his pension ledger lists his conditions as (i) GPI (agg); (ii) Double inguinal hernia (agg); (iii) Rheumatism (non-attrib & non agg); and (iv) neurasthenia (non-attrib & non agg). Ashman’s last address was the Glamorgan County Asylum, where he died on 22 August 1921. A married man, the risk would have been of his wife acquiring his illness.
How the assessing physician made the distinction in Ashman’s case between the symptoms of GPI and neurasthenia is unknown.
This diagnostic problem emerged in the following case:
- Pioneer (112001) Nathan Oakman, Royal Engineers was first diagnosed with neurasthenia (‘attributable’).This diagnosis was changed to GPI (‘aggravated’), 100% disabled. He had been rated 60% disabled in October 1920, then 40% in March 1921. Six months later he was 100% disabled and in Leicester Borough Lunatic Asylum, where he died in 1922. His symptoms had obviously progressed rapidly.
A curious pension decision was reached in four cases where the syphilis was deemed ‘attributable to’ service. What aspect of service involved contracting syphilis is open to speculation!
- Sapper (11345) Michael Bourke, 26 Field Company Royal Engineers, went to the Western Front on 17 August 1914. He was discharged on 14 January 1916, with a diagnosis of GPI. His syphilis was deemed ‘attributable’ to service (and he was evidently a Regular), and he was pensioned at 40/- a week. A married man, he died on 01/02/1920 in Killarney Asylum.
- Private (S/12708) Donald Henry Young, Seaforth Highlanders, was diagnosed with ‘degeneration, tabes dorsalis’ designated ‘due to’ service, rated 70% disabled. He had enlisted in February 1916 and was discharged in December 1917. His pension correspondence extends to 1927, 10 years during which he lived at five different addresses, and there is no death recorded.
(ii) Syphilis and gonnorrhea
There were 13 cases of syphilis and nine of gonorrhea amongst claimants. None were deemed attributable to service!
Multiple health conditions
Table 24 recorded that whilst 13,193 claimants were listed as having one or two medical conditions, 374 were diagnosed with three, 57 with four, and 1 with five.
Inspecting the pension ledgers, it is possible to form a negative view of the male nation’s health. Perhaps what is most depressing is that many men with pre-existing health conditions were selected for, and remained on, active service, despite the alleged weeding out. It is also notable that some received miserably low disability ratings and hence pensions.
One individual was pensioned with five medical conditions:
- Private (M/334058)Walter Bradshaw, Army Service Corps, was 28 when he was discharged in January 1918. His medal card suggests he served in the ASC (Motor Transport), enlisting on 11 December 1915, when he was working as a master decorator. Rated 40% disabled, he suffered defective vision (aggravated); aneurism (attributable); DAH (attributable); bubonocele (hernia – attributable); and enlarged thyroid (attributable).
The following images summarise the key details from Walter Bradshaw’s ledger pages:

Above: The first page of the ledger of Walter Bradshaw shows his name, regiment. Service number, rank, date of discharge, marital status, and address.

Above: The first page also lists his five conditions and whether attributable to or aggravated by service. It will be observed that the note ‘50%’ does not correspond with the ‘degree of disablement’ on the second page.
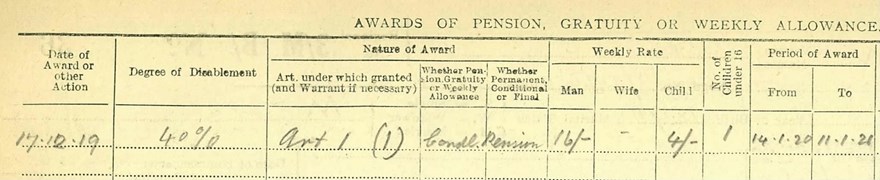
Above: The second page lists the date of the award, degree of disability, whether the pension was permanent, conditional or final (conditional in the case of Bradshaw), the weekly rate for man, wife, or child (16/- for Bradshaw, 4/- in respect of his child), and the period of the award (a year in Bradshaw’s case).
Fifty-seven men suffered with four medical conditions. The average disability was a curiously low at 29%. Seven were rated as 50% or above disabled, yet 26 were only rated as 20% or below disabled.
It seems difficult, once more, in some cases to understand why certain individuals were actually accepted for service:
- Private (35907) Jeremiah Coleman enlisted on 19 October 1914, aged 45, and was discharged in November 1917, having served in the Royal Defence Corps. (He enlisted on 19 October 1914 and must have served in some other unit previously). His pension ledger lists defective vision, debility, bronchitis and emphysema, all non-attributable/aggravated. He was rated 30% disabled. Given his physical condition, it might well be wondered how he was accepted even for the RDC.
Others showed a mix between attributable and non-attributable conditions:
- Private (17260) Edward Evans, Royal Warwickshires, was 46 when he was discharged in March 1919, rated 20% disabled. Rheumatism and asthma were deemed ‘attributable’ to service, and debility and elbow ulceration ‘non attributable and non-aggravated’.
- Private (130170) Samuel John Chaney, Labour Corps, had previously served as Private (12521) South Wales Borderer. He had suffered a GSW to the head. However, he also suffered debility following dysentery (attributable); rheumatism (non-attributable); bronchitis (attributable); and malaria (attributable). Discharged in September 1918, aged 30, he was rated 40% disabled a year after discharge, and 6-14% two years later (weekly pension 13/6d).
Some soldiers were pensioned for conditions deemed attributable to service yet had low disability ratings that seem hard to understand:
- Corporal (40013) Charles Manley, South Wales Borderers, was 30 when he was transferred to the Special Reserve in March 1919. His conditions were listed as DAH, anaemia, tachycardia, and pneumonia with debility, all attributable to service, yet was rated as only 1% disabled, awarded a miserable 6/- a week, with a £5 gratuity when he was rated as 0% disabled in March 1920.
- Gunner (13349) Morgan Collins, Royal Field Artillery, was pensioned following discharge in December 1918 for pleurisy (non-attributable); DAH, fractured pelvis and malaria. These conditions were all deemed ‘attributable’, as was a further diagnosis of neurasthenia. He was rated as little as 20% disabled (pension of 9/6d).
- Sergeant (3034) William Robertson, Royal Field Artillery, a blacksmith who had joined up in 1900, was 40 when he was transferred in September 1918. He was pensioned for malaria, bronchitis, asthma, dysentery and inguinal hernia, all attributable to service. He had also sustained a GSW to the face, yet was rated as only 20% disabled (pension of 9/4d with 7/- for his wife and four children).
Other soldiers, in comparison, received relatively high disability rating:
- Private (R4/066524) John D’Arcy, Army Service Corps, was 29 when he was discharged in June 1919. His disabilities were debility (attributable); deficient teeth (aggravated); TB (attributable) and malaria (attributable). A year after discharge he was rated as 20% disabled, then 60% in December 1921 as his TB progressed. His final disability was rated at 50%. Correspondence continued to 1932, at which point he died.
- Sapper (323190) James Farrell, Royal Engineers, was 48 when he was discharged in September 1919. He was pensioned for malaria, ‘shedding teeth’, pulmonary TB, and bronchitis. From November 1919 he was variously rated as 50%, 20%, 30%, 60%, 100% and 60% disabled, before dying in February 1923.
- Private (2038) Patrick Cahill, 5th Battalion Royal Irish Regiment, was 40 when he was discharged in October 1919. He had enlisted in November 1914, but had previously served in the 2nd Connaught Rangers and 2ndLeinsters (discharged ‘with ignominy’ for desertion a month before the war’s outbreak). His records show further court martials for various ‘crimes’, including absence and theft. He went to the MEF in July 1915 and the EEF in 1917, returning to the UK in June 1918. He was pensioned with malaria, varicose veins, hydrocele, and pulmonary TB, all deemed attributable. He was rated 100% disabled.
4. Psychological Conditions
Overview
The psychological effects of service in the Great War remains a controversial subject. Alex Watson observes that ‘most men clearly overcame battle stress extremely successfully’.[118] From about five and a half million British soldiers who served, the much-criticised official figures presented in Diseases of The War describe 28,533 shell-shock battle casualties to the end of 1917. A maximum 80,000 cases of ‘nervous disorder’ was finally arrived at.[119] Peter Leese suggests that it is currently estimated from studies of the French and German armies that a more reliable overall figure for cases of psychological disorder is around 200,000 – even with this revision, Watson’s point seems well made.[120]
Predictably, however, in our modern world increasingly preoccupied with the concept of trauma, such estimates have been amplified. Jay Winter, pushing the boundary of Second World War combat stress estimates,[121] plucks from the air a figure of 20 per cent of all Great War casualties being psychiatric in nature, suggesting ‘a band of probability’ with its lower end at 4 per cent of all casualties and at its upper end at 40 per cent, concluding: ‘A mid-point could be the best approximation we can offer.[122] Based on Leese’s review, however, the figure would in fact be just under nine per cent of all casualties.[123] If this is correct, the fact is that there were relatively few psychiatric casualties, rather than so many. The coping skills of the time clearly proved effective.
In a recent book on shell shock, Suzie Grogan wrote that it was important ‘to acknowledge that not everybody exhibited the classic signs of emotional distress linked to war trauma’. She noted that many soldiers returned from war ‘exhausted, drained, but essentially in one piece physically and mentally’. She went on to optimistically state that many ex-soldiers ‘went on to live happy and fulfilling lives’.[124] This view is undoubtedly correct. The desire to acknowledge the ordeal of the First World War soldier is not appropriately fulfilled treating shell shock as a synonym for suffering.
It would be easy for our desire to recognise this suffering to allow us slip into a place where we view Great War veterans as inevitably perpetual victims of their experiences. A good example of the distortion induced by using present-day expectations to anticipate reactions of a century ago is the retrospective use of the symptom-set of Post-Traumatic Stress Disorder (PTSD) to frame veterans’ reactions. Re-experience phenomena, including flashbacks (involuntary, vivid images of the traumatic event which occur in the waking state) and nightmares are a hallmark of the diagnosis. Modernity expects the Great War soldier’s peace to have been riven by flashbacks and nightmares. It is interesting, therefore, that in a study of war pension files, only half a per cent of 567 First World War veterans reported flashbacks.[125] Indeed, at the time, Professor Graham Brown reported that in the Salonika force, only five per cent of men under fire had nightmares.[126]
There seems good reason to believe that the expression of trauma is different not only between cultures, but at comparatively close points in time within the same culture. In respect of re-experiencing, it has thus been suggested that the prevalence of moving visual imagery in the form of film in modern life has encouraged people to have more visual representations of everything, including trauma. As moving imagery became more a part of everyday life, memories became more visual.[127]
The reality of the First World War was, of course, that at points when coping wore so thin that it was no longer effective, psychological symptoms emerged. Such episodes were, however, often temporary. The majority of soldiers affected returned to duty. Removal to a base hospital, especially in Britain, produced a poor return rate. Of a series of cases of nervous disorder from November 1916 to May 1917, sent to a neurological centre in France, however, 65 percent so returned.[128] A Casualty Clearing Station operating in December 1916 produced almost identical figures – sixty-six per cent of 200 returned to ‘the firing line’ after seven days.[129] Charles Myers had established four special shell-shock centres close to the front-line by the end of that year, and the return to duty rate rose from 50 per cent to 90 per cent.[130] During Third Ypres in 1917 Gordon Holmes claimed that overall 80 per cent returned to duty within two to three weeks.[131]
There is no doubt some truth in Holmes’s assertion that many men who were sent down from the front line were ‘merely shaken up’, and that these individuals ‘slept for 24 hours and after a few night’s good rest’ were largely recovered.[132] Whilst there is evidence that the army inflated the return rate from hospitals, these particular figures are consistent with more recent experience.[133] What we do not know with clarity is how many men across all the studies returned to combat roles. A current estimate of rate of return to duty after psychological treatment is that ‘most servicemen can be returned to duty, although fewer than half go back to combat units’.[134]
It is important neither to overestimate nor underestimate the prevalence of psychological casualties. To overestimate reflects an undervaluing of soldiers’ coping mechanisms. To underestimate would be to downplay the destructive nature of the war on the human psyche. Peter Leese suggests that there were ‘neurotic ex-servicemen’ who though affected during the war recovered quickly in its aftermath. This is what would be expected from a positive view of soldier’s coping mechanisms. Yet, there were similarly those who did not recover.
With a narrow focus on the war, it would be easy to assume that it was necessarily the sole factor in breakdown. The men who went to fight had previous personal characteristics to be taken into account, and for some, these included a vulnerability to breakdown. In a study of hospitalisation in Salonika, 49 per cent of psychiatric casualties had a history of pre-war ‘neurosis’.[135] The fact that the more vulnerable had an increased risk of breaking down in the face of war is in itself nothing surprising. It appears a cruel thing to have sent vulnerable individuals to war, but it is simply a sad reflection of the absence of appropriate selection. As Peter Barham has noted, many of those who remained in psychiatric hospitals for the rest of their lives after the war were those with previous histories of mental illness.[136]
in an era preoccupied with degeneracy, Jones and Wessely note that ‘it was the widespread nature of shell shock and other war syndromes during the First World War that helped to undermine the traditional distinction between the hereditarily fit and unfit. When officers were found to suffer disproportionately from the disorder, mental illness could no longer be conceived in the restricted realm of degenerates and weak hereditary constitutions’.
Psychological conditions in the pension ledger study
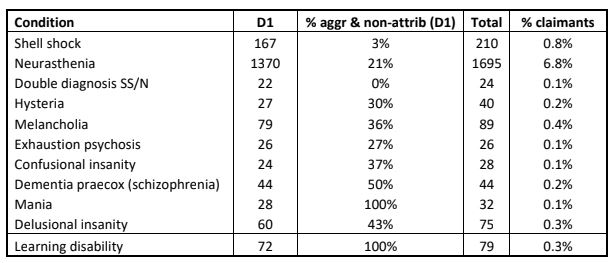
Table 31:Overview of psychological conditions in the PLS (D1 = psychological condition first listed)
In the PLS, claims for psychological disability made up 9.3% (2,330 cases) this being virtually identical to this writer’s observation that psychological conditions likely accounted for just under 9% of casualties. However, if the PLS is truly representative of the 1,600,000 pensioners, then the total number of diagnosed psychiatric casualties who were pensioned would be just over 149,000, i.e. below Leese’s projected figure of 200,000. Eighty-two per cent of these were where a psychological condition was the first or only listed. What we do not know, however, is how many psychiatric/psychological conditions underlay other pensioned conditions such as DAH. Nor do we know, however, how many servicemen suffered in silence.
Table 31 shows all the various diagnoses recorded. Excluding learning disability, there are 1,869 pensioned psychological casualties, where such is listed as the first condition, of which 85% comprised shell shock, neurasthenia and hysteria, and the remainder serious mental health conditions which in the modern era would be described as ‘neurodevelopmental’, resulting from interaction between genes and environment, of which latter psychosocial stress would be one aspect.
This is not the place for a review of the whole concept of shell shock and neurasthenia. The OH (Diseases) groups psychological symptoms into four categories: (i) simple exhaustion, (ii) neurasthenia and anxiety, (iii) hysterical states; and confusional states. The ‘neurasthenic group’ comprised some 60% of cases overall (although comprising 81% of pensioned cases in the PLS). The OH lists as symptoms ‘headache, dizziness, failing powers of concentration, inefficient memory for details, a sense of helplessness when faced with the necessity of making an effort, a constant state of irritability, and irregularity of sleep associated with nightmares or a riotous mental activity during the night. Behind all these, too, there existed a continual state of dread and anxiety.’ A separate definition of ‘shell shock’ was not made. It is interesting that the OH noted: ‘true malingering was very rare and could only be definitely proved in a few cases’.
The Ministry of Pensions studied two groups in 1921 (N=16,393) and identified three classes of cases: (i) ‘definitely attributable to shell shock, i.e. explosions’ (31%); (ii) ‘due to general war stress (emotion)’ (61%), with a further group of 6% developing after discharge; and (iii) ‘cases due to social and family conditions in financial distress’ (2%).What is interesting in the PLS, whose diagnoses were largely made/confirmed post-1918 is that only 16% received shell shock diagnoses, the rest being neurasthenia. This reflects the OH’s subsuming of shell shock within the ’neurasthenic group’.

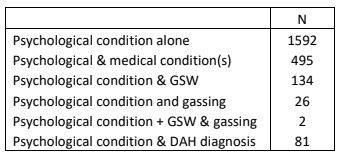
Table 32: Range of psychological and associated pensionable conditions
Table 32 is interesting as it demonstrates the low linkage between psychological conditions and wounds – a psychological condition was three times more likely to be associated with a medical condition that wounding.
In their PIN26 study (southern region) of WW1 pensions Jones et al found neurasthenia/shell shock/anxiety neurosis/nervous debility/depression made up 4.3% of pensions as a sole diagnosis and 5.8% as part of a multiple diagnosis.[137] This adds up, obviously to 10.1% and is comparable to the 9.3% found in the PLS.
Shell shock
Jones and Wessely[138] observe that with respect of shell shock no unambiguous definition of the condition exists. The report of the shell shock committee in 1922[139] described it as ‘emotional shock, either acute in men with a neuropathic predisposition, or developing slowly as a result of prolonged strain and terrifying experience, the final breakdown being sometimes brought about by some relatively trivial cause. (Or) nervous and mental exhaustion, the result of prolonged strain and hardship’.
Importantly, Jones and Wessely caution against seeing shell shock as ‘the cultural predecessor of PTSD’. They emphasise that shell shock is ‘one example of a variety of functional somatic disorders’ rather than simply a psychological condition in its own right.
In a series of 50 Army claimants with a sole pension claim of diagnosed ‘shell shock’ (of which there were only 167 in the PLS), the average disability was 28%. This was a reduction from 43% on first assessment recorded on the pension ledger. Two were rated as 100% disabled with eight rated 50% disabled or over. Twenty-eight were rated as 20% or below disabled. All were described as ‘due to’ service, yet as Table 31 shows, 3% overall were regarded as ‘aggravated’ or ‘not attributable’, which might be viewed as curious given the diagnosis applied, but which becomes more understandable given the later consideration of this diagnosis under the ‘neurasthenia’ umbrella.
Within this series of 50, three have extant pension records which allow us to understand their symptoms.
- Lance-Corporal (2023) Walter Newcombe, Berkshire Yeomanry, was discharged on 21 February 1917, aged 27, and pensioned for ‘shell shock’, rated ‘60% then 50%’ disabled (16/6d then 13/9d per week). A gamekeeper by profession, he had enlisted on 7 September 1914, and his character as a soldier was described as ‘very good’. He had spent 162 days with the Mediterranean Expeditionary Force in 1915.‘Patient states that in August 1915 in Gallipoli, he was blown up – his right knee being injured & he states that he felt dazed for some days after it. Admitted Reading War Hospital 17/9/15 with internal derangement knee joint, discharged 8/10/15.’ Admitted Kitemoor Aux. Hosp. with shell shock discharged 1/1/16.’ Following this his knee was operated on and cartilage removed. (This injury is not listed on his pension ledger record). In terms of his shell shock symptoms: ‘Patient is very nervous. There is marked muscular tremor. He complains of headache, dizziness and occasional fainting after any exertion or excitement. He also complains of shortness of breath on exertion. The heart is neurotic’.
- Private (79939) John William Markham, Sherwood Foresters, was 23 when he was discharged on 4 July 1917 as a result of ‘shell shock’. He had enlisted in May 1913 in the 6th Battalion, his profession being a collier. He was rated 20% disabled in June 1920 (weekly pension 5/6d).Serving on the Western Front from 28 February 1915, his injury dated from 1 July 1916 at Gommecourt, when he was buried by an explosion. He was hospitalised in the 4th London General Hospital from 14 July to 26 September 1916 – ‘usual symptoms, treatment in neurological section’. He was subsequently transferred to No. 6 Agricultural Company. On discharge he was described as: ‘’Shaky, headache, sleeps badly … slight tremor of hands and speech’. In April 1918 it was recorded: ‘Somewhat tremulous, and complains of headaches’. In February 1919 the doctors was more expansive: ‘Knee jerks exaggerated, pupils sluggish, fine tremors hands, short of breath, pain frontal region.’ His pulse was 150. Fourteen months later he still complained of headaches ‘especially after a heavy day’, adding ‘nervous in company … trembling and shaking’, although his ‘mentality’ was described as ‘hopeful’.
- Private (5700) Arthur John Dyer, Lancashire Fusiliers, was 29 when he was discharged on 16 February 1918, with ‘shell shock’, finally rated 15-19% disabled (weekly pension of 10/6d, the pension for his wife and two children removed).His condition originated at Fricourt on 7 July 1916. A colliery haulier, he had enlisted on 5 September 1914 and had been on the Western Front 15 September 1915 to 27 September 1915, and 25 February to 8 July 1916. He was hospitalised from 9 July to 28 August at the 2nd Western General Hospital, Manchester (where he also went down with ‘flu). He was described as ‘much improved since discharge. Now fit to resume some light work in civil life’. He had originally been rated 40% disabled, ‘very shaky, reflexes exaggerated, stammer very bad’. In July 1918 it was recorded: ‘He is very nervous & tremulous. His speech is much affected but improving. Sleeps badly. Pale & anaemic. DAH, tachycardia 125’. When seen in March 1919 his blood pressure was raised and there were abnormal heart signs. A year later it was recorded: ‘Is very nervous. Stammers’, but it was now noted ‘sleeps well’. His general condition being ‘good’, he was downgraded to 20% disabled. Six months later, however, it was noted once more: ‘Is very nervous, gets attacks of dizziness. Gets pain in R side. Stammers a good deal’. In October 1922 his heart appeared normal, but there were ‘tremors under examination’, and he was now noted as ‘dull, educational attainment sub-normal. Moderate initial stammer’. ‘Neurasthenia’ was now recorded (but not on his pension ledger record), with 15-19% disability.

Above: The alleged ‘1,000 yard stare’ of shell shock
As might be expected, disability ratings dropped over time:
- Private (3540) James Brewer, Leinster Regiment [and Private (4683399) KOYLI] was 25 when he was transferred to the Reserve in May 1919. He went through a diagnostic change – firstly ‘insomnia’ and ‘melancholia’ and subsequently ‘shell shock’. He was rated 60% disabled in September 1919; 40% in July 1920; 20% in June 1921 and finally 6-14% a year later. Clearly he was improving, whatever the correct diagnosis.
- Gunner (695732) Charles Hardman was 28 when attested in 4thCheshires on 25 January 1915, but was discharged ‘on account of bad teeth’ to the West Lancashire Divisional Ammunition Column in March 1916 (where his elder brother was serving).He later served as a Driver for 12 Brigade Royal Field Artillery on the Western Front from 5 July 1917 until 29 November that year. He was transferred to the Army Reserve on 19 June 1918. ‘Steady and hard-working … sober and reliable’, it is interesting that as a Birkenhead rigger he was returned at this point to shipbuilding (rather than transferred to the Labour Corps). As he was pensioned on transfer, it must be presumed that it was his shell shock that had led to his return from the Western Front and his discharge. In March 1920 he was viewed as 60% disabled, dropping to 40% a month later (pensioned at 16/- per week, with 9/5d for his wife and children). His four year old son had died in August 1917 of pneumonia, some six weeks after he went on active service. His case makes one wonder as to what role the death of his son played in his psychological decline, and how he coped with the noise of a shipbuilding environment.
- George William Clutterbuck, a 45 year old labourer when he attested on 26 November 1915, served first as (PW/4215) in the 26th Battalion Middlesex Regiment (destined to be Pioneers). He was, however, discharged 11 days later ‘unfit for military service suffering from lung disease’. He reappeared as Pioneer 162122, Royal Engineers, Railway Troops Depot, enlisting on 6 May 1916 (presumably conscripted), and discharged on 3 May 1917 due to ‘shell shock’. The amount of time he spent on active service is not known. He was rated as 70% disabled in June 1920, 60% a year later, and finally 30% disabled in September 1922. Either there was lack of joined-up thinking in relation to his previous discharge, or it was thought acceptable to put this vulnerable man into non-teeth services, a matter reflected by his development of shell shock on lines of communication work.
Neurasthenia
The OH (statistics) claims that ‘in cases of true “war” neuroses (i.e. those manifested in men with a minimal predisposition) the symptoms rapidly disappeared on the cessation of exposure to war conditions’.[140] In those with ‘a fairly well-marked predisposition, the subsequent progress depended largely on the environment and conditions to which the men were afterwards subjected’.
As Table 31 shows, 79% of neurasthenia conditions were viewed as attributable to war service. They showed some latency, whereas psychoses showed more marked latency. In a series of 50 Army claimants with a sole pension claim with diagnosed ‘neurasthenia’, the average disability was 24%. This was a reduction from 31% on first assessment recorded on the pension ledger. None were rated as 100% disabled with five rated 50% disabled or over (the highest being 60%). 29 were rated as 20% or below disabled. A few cases in this series were diagnosed as ‘mental instability’, ‘anxiety neurosis’ or even ‘nervousness’.
Three cases provide a picture of the symptoms.
- Sergeant (S4/143308) William Dent, Army Service Corps, was 42 when he was discharged in January 1919. His neurasthenia was deemed attributable to service, and he was rated initially 50% then 40% disabled. In December 1920 this had decreased to 30%. A butcher in civilian life, he had enlisted in October 1915, and had gone to the Western Front in February 1917. The origin of his neurasthenia was dated to March 1918. Examined at the Maudsley Hospital (where he was in inpatient for 2 and a half months at the end of 1918) it was noted ‘C/O pains in legs. Weakness. Hands all a tremor. Occasional headaches, Pupils unequal’. He suffered facial paralysis initially (presumably a hysterical reaction). This appears a very physical examination. When examined in Darlington on 16/5/1919 it was observed: ‘He is emotional. Tremors are marked. Twitching of islets. Pupils react to light and accommodation. Has more control of himself’. He was rated as 50% disabled. On 21 November that year it was further noted: ‘Restless at night. No war dreams. Concentration bad. Memory impaired. Nervous in dark and of loud sounds in traffic. Restless … at home. Fine tremors hands and eyelids (rated 40% disabled). He was observed to be working in the open-air. Later he was still recorded as: ‘Nervous if alone. Better in company. Nervous in dark. Apprehensive, restless and irritable. Fine tremors.’ A further year on the doctor wrote: ‘Neurasthenia due. C/O nervousness, easily startled. Temporary casual clerk in labour exchange. Unfit at the moment.’ He had been able to progress from outdoor to indoor working and was now rated 30% disabled. In November 1922, a Special Board noted: ‘C/O nervousness and afraid of walking in dark, headaches frontal. Sleeps for hour then wakes up. Can’t do work as butcher, afraid of the cattle. Dreams, can’t remember them, occasionally of being in army. Rises early, does a bit of work in garden. Does not like company or amusements. Can’t put attention in reading. Apprehensive of harm. Coarse and fine tremors of hands and fingers. Prematurely grey. Worried expression. Memory and reaction time normal. Emotional. Subdued.’ He was finally rated as 30% disabled.
- Driver (74492) Thomas Hughes, Royal Field Artillery, was 26 when he was discharged in June 1919 with neurasthenia. He had joined the Special Reserve in 1913, when he was a gas works labourer, but at the outbreak of war was a machine driller for Armstrong Whitworth. He served on the Western Front for four years. He was rated 70% disabled on discharge, 60% in December 1919, 60% a year later, 40% in July 1921, 30% in January 1922, and finally 20% at the end of that year. The origin of his disability was dated to 17 September 1917 at Ypres – which ‘he attributes to gun fire bombardments’. He was treated at the 1st Northern General, Newcastle (50 days); and the Gateshead War Hospital, Stannington (132 days), ‘admitted with history of dizziness under heavy fire. Went sick when home’. He had been granted leave on 15 August 1918, and had been admitted first with ‘nervous debility’. It was noted: ‘Very depressed – looks melancholy, has tachycardia, vertigo, headache, pains in back and legs, insomnia. Is very slow in speech and thought. Has attacks of perspiration frequently, has frequent night starts, has also claustrophobia. Is very anaemic and debilitated. No valvular lesion in heart. Lungs normal’. Later it was recorded: ‘Dreams a lot, terrifying dreams, cannot stay alone. Speaks in low listless tone. Markedly depressed and tremulous. Heart normal. States he cannot do his work nor concentrate his mind on anything. Fine tremors’. It was noted on discharge from Stannington: ‘All symptoms clear and now fit for work’, and, interestingly in 1925 it was recorded ‘man in Belgium’.
- Lance-Corporal (99512) Alexander Innes, Machine Gun Corps, a pre-war drapery assistant, was 24 when he was discharged in February 1919, 30% disabled (initially 40%) with neurasthenia. He attested in February 1916, and served on the Western Front from 15 July 1917 to 22 September 1917. The origin of his disability was on 22 August 1917. ‘Was in line at Ypres & Messines Ridge when he was shell shocked being blown on to parapet. Was very shaky but carried on for a few days. Became very confused & was eventually sent into hospital’. He went first to 16 General Hospital at Treport, and returned to the UK to a series of institutions: ‘White Cross Warrington; Caernarvon; Winwick and Stannington.’ He was ‘very nervous, giddy, headaches, fatigue on small exertion, tremors, terrifying dreams & insomnia’. In February 1919 it was noted: ‘Free from nervous signs and symptoms, but is of neurotic tendencies’. (His pension ledger indeed states ‘aggravated’). He married in November 1918, and emigrated to Australia in 1920.
Lastly, a puzzling case from the point of view of a pension award:
- Private (567133) Andrew Gribben (or Gribbin), Labour Corps [and previously Private (24659) King’s Own Scottish Borderers] was discharged in March 1919, rated 20% disabled that October. His pension ledger lists ‘debility’, ‘GSW leg & back’, and ‘heart trouble’. These items, all ‘due to’ service are crossed out, and neurasthenia added (with no indication of attributability), seemingly remaining the single pensionable condition. It seems unlikely that the first three noted conditions were not the cause of his transfer to the Labour Corps, and further unlikely that they ceased to trouble him.

Above: Still from ‘War Neuroses: Netley Hospital (1917), pt. 1 of 5’ Wellcome Collection (CC BY-NC-SA)
Double diagnosis shell shock/neurasthenia
As noted in Table 31, there were 22 cases of a double diagnosis of shell shock and neurasthenia. The discussion above sets out that by the time the OH came to be written, there was reference to a ‘neurasthenic group’, with shell shock essentially subsumed into neurasthenia. Comparing the three cases of shell shock diagnosis with the three of neurasthenia presented above, it might be thought that the diagnosis could be switched in each case.
The average disability on first rating was 39%, and the final rating was 28%, very similar to the figures obtained from those with a single diagnosis of ‘shell shock’. There is no indication therefore that these cases represented a more serious condition.
One case of double diagnosis suggests good recovery:
- Private (3191) James Johnstone, Ayrshire Yeomanry, was 23 when he was discharged on 1 January 1917. He had enlisted on 10 August 1914. The duration of his service overseas is not known. His pension ledger is remarkable in the it is one of the very few which uses the word ‘traumatic’. The three conditions on his pension ledger are (1) Shell Shock, (2) Traumatic (3) Neurasthenia, all ‘attributable’. He was rated 70% disabled in November 1919, but only 1-5% in November 1922. He died in 1924, cause unknown.
Hysteria
Hysteria as a condition was far more widely recognised at this period in time by German and French psychiatrists. With the view that it was particularly associated with women, the high valency of ‘manliness’ in British society meant that it was a less favoured diagnosis.
Hysteria is now known as ‘Conversion Disorder’ (estimated with a minimum prevalence in the present era of 48 per 100,000).[141] It is a functional neurological disorder, i.e. a physical condition for which no physical cause can be found. Typically, this disorder affects movement or the senses, such as the ability to walk, swallow, see or hear. Symptoms can vary in severity and may come and go or be persistent. The individual cannot intentionally produce or control their symptoms. It might be observed that more dramatic cases of shell shock shared aspects of this condition.
There were 27 cases of hysteria. Where more information is given in the ledger, the case is described below. Of the 12 cases where further information is available, ten involve mobility.
- Private (61138) James Alves, 19thBattalion Middlesex Regiment was 31 when he was discharged in September 1918, having enlisted in May 1917. In March 1920 he was rated 30% disabled, dropping to 20% seven months later (pensioned at 8/- per week with 5/11d for his wife and 3 children). He was first diagnosed with ‘hysterical paraplegia’ and ‘war neurosis’. He thus suffered a hysterical paralysis to the lower parts of his body. These two entries are crossed out, and a diagnosis of ‘neurasthenia’ substituted. We must presume that the paralysis remitted, leaving him with more general psychological symptoms. In 1939 he was working as a tailor.
- Private (8808) Herbert Abbott, 1st Battalion Northamptonshire Regiment, was 23 when he was discharged on 20 May 1915 with paraplegia. A Regular soldier, he went to France on 13 August 1914, and would have seen action on the Marne and Aisne, and during First Ypres. The diagnosis of paraplegia is crossed out and ‘conversion hysteria’ (attributable) substituted, it being subsequently recognised that his condition was psychological in nature. In April 1920 he was rated 40% disabled, reduced to 30% in September 1922. In 1939 he was working as a joiner.
There were a further four cases noted as similar to Herbert Abbott’s:
- Private (8246) William Hetherton, 1st & 2nd Battalion Royal Irish Fusiliers, who had arrived in France on 22 August 1914, was 37 when he was discharged in November 1917, diagnosed with ‘hysteria hemiplegia’ (hemiplegia being a severe or complete loss of strength or paralysis on one side of the body). He was first diagnosed as 50% disabled, and finally, in April 1922, as 30% (pensioned at 12/- per week).
- Private (105961) Thomas Eagles, RAMC, who had enlisted in December 1915, was 29 when he was discharged in January 1919, diagnosed with ‘hysterical contracture of the right knee’ (i.e. he could not bend his leg), rated 10% disabled. In 1939 he was working as a ‘stage door keeper’.
- Private (53751) Frederick Charles Attack, Manchester Regiment, was 23 when he was discharged in November 1918. He had been wounded in the leg, but was pensioned (less than 20% disabled) for ‘functional foot drop’ in the affected limb (‘attributable’, 5/6d per week).
- Private (369) Thomas Dorrington, 11th Field Ambulance RAMC, was discharged in June 1916, aged 38. He had gone to France on 24 August 1914, but was discharged with a diagnosis of ‘hysteria (paralytic, anisthetsic (sic)’. Hysterical anaesthesia is inability to feel pain, and in Dorrington’s case, was evidently combined with paralysis). In January 1920, he was rated 100% disabled, and his disability rating only dropped in May 1922 to 30%, when presumably he had showed considerable recovery (the award to his wife being cancelled at this point as presumably the burden of care was reduced). Five months later, he was rated 40% disabled (pensioned at 16/- per week). His condition was first viewed as ‘attributable’, but later changed to ‘aggravated’.
- Gunner (127442) Arthur Okey, RFA, was 20 when he was discharged in December 1916. He was diagnosed with ‘hysteria epilepsy’ (‘aggravated’), rated 20% disabled.
- Rifleman (5284) William Abbott, Rifle Brigade, was 24 when he was discharged in December 1917, having gone to the Western Front in September 1915. He was diagnosed with ‘functional aphonia’, i.e. he had ceased to speak. He was diagnosed 70% disabled in march 1920 and ‘less than 20%’ in November 1922 (pension 7/6d per week), when presumably his speech had recovered but psychological issues remained. He died 10 years after this last assessment, cause unknown.
Neurodevelopmental conditions
Overview
Six principal neuro-developmental conditions were identified.
Melancholia (a term rarely deployed currently) is a more severe type of depression, with physical symptoms, frequently referred to as endogenous depression in more modern times. It is assumed to have a primary biological causation. Melancholia formed 20 percent of 1910 Cardiff Mental Hospital admissions and 12 per cent of Hereford Lunatic Asylum admissions.[142]
The remaining conditions, confusional insanity, Dementia Praecox (schizophrenia), mania and delusional insanity are all different types of psychotic phenomena. In 1910, cases of delusional insanity made up 20 per cent of those admitted to the Cardiff Mental Hospital and 21 per cent of the admissions to the Hereford Lunatic Asylum.[143] These illnesses are similarly assumed to have a primary biological causation.
In 1880, one Dr Sptzka defined ‘primary confusional insanity’ … a form of mental illness ‘which develops rapidly on a basis of cerebral exhaustion. Consciousness is blurred in parallelism with the conceptional disturbance and the patients on recovering have, as a rule, but very crude recollections of their condition. Its duration is variable, comprising weeks and months. The prognosis is, as a rule, as good as that of stuporous insanity’.
Dementia Praecox was the old term for schizophrenia. This condition will emerge in up to 0.7 per cent of the population between the late teens and early 30s (the two cases were 24 and 29), with symptoms of hallucinations, delusions, disorganised thinking, withdrawal, decreased emotional expression and apathy. Whilst probably about a fifth of asylum admissions in the early part of the 20th century were such cases, British psychiatrists were slow to accept the concept, and patients were often given other diagnoses.
Exhaustion psychosis is most frequently seen as a phase of a significant psychotic episode. It is an acute state of confusion and delirium that occurs in relation to extreme fatigue, chronic illness, or prolonged sleeplessness. This demonstrates the interaction between the biological underlay and the environment.
In their PIN26 study (southern region) of WW1 pensions Jones et al found manic-depressive psychosis/schizophrenia/psychosis made up 0.3% of pensions as a sole diagnosis and 0.3% as part of a multiple diagnosis.[144]
Melancholia
Seventy-nine soldiers were diagnosed with melancholia, the largest number of all the neurodevelopmental conditions. Thirty-six per cent of cases were deemed aggravated/non-attributable.
That this was a significant illness is illustrated by the following case:
- Private (422354) Robert Andrews, Army Service Corps, was 43 when he was discharged in September 1919. The severity of his melancholia (deemed ‘attributable’) was indicated by the fact that he was rated 100% disabled, and his address was given as the County Asylum, Bridgend. He died in August 1923.
The fact that the condition bordered on psychosis is indicated by the following case:
- Private (29/842) Charles Ahern(e), Royal Irish Regiment, born in 1890, was discharged in January 1918, with a diagnosis of ‘acute melancholia’ (‘attributable’). He was rated 60% disabled in September 1919 and 70% in June 1922. Previously a farm labourer, he had served pre-war in India with the 1st Battalion Royal Dublin Fusiliers, described in 1911 as ‘slow, slovenly, and not overwilling’, and was a reservist on the outbreak of war. Posted to Gallipoli with his old unit (16/03/1915 to 01/10/1915) he was invalided following a GSW to the left shoulder. Transferred to a Home Service Garrison Battalion of Royal Irish Regiment, he was court martialled in June 1917 for ‘when on active service striking a soldier’. His melancholia symptoms, the basis of this incident, formed the basis of his pension claim (his shoulder wound did not appear on his pension ledger). ‘According to his own statement he was suffering from headache, dizziness and noises in his head and he believed that other soldiers were laughing at him … the result was that he assaulted a soldier’. He was treated in the King George V Hospital, Dublin, for over 6 months, where ‘ he was very dull and depressed & complained of headache, buzzing noises and persecutory delusions, imagined people were laughing at him. He complained of insomnia. He perspired about the head and had a sensation of being stabbed from behind in the neck. Memory very defective’. He was ‘tremulous’ and ‘nervous’. He was paranoid about his fellow patients. On leaving hospital, he had ‘lost his hallucinations and delusions’, but was now described as ‘weakminded and would be likely to break down under strain of military service’. Attributability was ‘stress of campaign, & being buried & wounded’ (although ‘buried’ may actually have been a fall).
Another case gives an example of a Regular soldier whose melancholia was not attributable to military service, yet who was kept within the Army despite his problems before the war:
- Private (9394) Patrick Hannafin, Royal Munster Fusiliers, was discharged in April 1915, aged 23. A butcher, he had originally enlisted in 1910. He was diagnosed with melancholia (recurrent – agitated) and there is a note on his ledger stating ‘pre-war pensioner’. His illness was not deemed attributable to service. He was described as ‘depressed, reclusive … complains of noises in the head at night’. Further, he stated ‘his head swells in the summer and he gets big bumps on it’. At night he ‘hears noises driving “bad morals” into his head & telling him to go to America’. He was rated 70% disabled in 1915, and 60% in June 1921.Pre-war he had first been posted to the East Indies, but had returned to the UK after being in ‘detention’. It seems possible this was the first indication of his troubles, yet he was then sent to Burma. The examining doctor noted in March 1914 in Rangoon: ‘I can find no trace of insanity in his family’ but ‘he is said to have tried to hang himself from the ceiling of the company bungalow’ and ‘would do it again if given another chance’, and, indeed, he tried to drown himself. ‘Unfit for further service’ was the conclusion on 20 August 1914, yet his final discharge was from Netley having arrived from Rangoon in March 1915. How he could have been a pre-war pensioner, which his records seem to indicate, is unclear.
Exhaustion psychosis
Exhaustion psychosis is sometimes referred to as ‘mental stupor’ in the pension ledgers. There were 26 cases recorded, of which 27% were regarded as aggravated/non-attributable. Whilst no detailed pension records exist for the 26, the following case indicates a reasonable recovery for the individual involved:
- Private (10666) William Joseph Deegan, 4th Hussars, entered France on 17 May 1915, and was discharged with ‘exhaustion psychosis’ on 7 November 1918. His condition was described as ‘aggravated’. He was rated 60% disabled in September 1919, but only 6 to 14% in May 1921.
Confusional insanity
There were 24 cases of confusional insanity, 37% regarded as aggravated/non-attributable.
- Driver (800744) Charles Pick, RFA, was 22 when he was discharged on 2 November 1918, with confusional insanity, ‘aggravated’. He had arrived on the Western Front in February 1915. He was rated 30% disabled in February 1919, 20% in May 1920, and 15-19% in March 1921. His condition was described as ‘Weakminded. Eccentric in his conduct … Loss of memory, irritable and emotional.’ He was treated in Murthly War Hospital from 10 May 1918 until his discharge. Here it was noted: ‘He has had a relapse when he threatened suicide. There is hereditary predisposition to insanity – father being insane. He appears to have made a good recovery, but too unsuitable for further military service’. A pre-war labourer, in 1939 he was working as a labourer in a foundry.
- Private (13918) George Paul Dickie, 1st Scots Guards, was 24 when he was discharged in June 1917. He had enlisted on 11 May 1915. He was discharged with diagnoses of ‘confusional insanity’ (‘aggravated’) and ‘locomotor ataxia’ (‘aggravated’). He was rated 80% disabled. As the latter condition represents loss of coordination of movement, especially as a result of syphilitic infection of the spinal cord, one wonders whether Dickie had been given the correct diagnosis.
Delusional insanity
There were 60 cases of delusional insanity, 43% viewed as aggravated/non-attributable.
- Private (7733) Michael Fitzgerald, South Lancashire Regiment, was born in 1884 and had attested in 1904, when he was a dock labourer. An unruly soldier, he had convictions under both military and civil powers. A reservist, he was mobilised on 5 August 1914. He sustained a GSW to his right hand in October 1914 in France, which is not mentioned in his pension ledger. He was first diagnosed with ‘melancholia – permanent – attributable to service during present war’, later changed to ‘delusional insanity’. He was rated 100% disabled, and confined to the District Asylum, Limerick.
Two cases indicate how the war wove itself into men’s delusions:
- Private (35291) Bert Harvey, 13thBattalion Royal Welsh Fusiliers, was discharged in May 1918 aged 28. ‘A steady, sober, honest, industrious man’, he served on the Western Front from May 1916 for 1 year 47 days. He had enlisted in December 1915. He was admitted to 130th Field Ambulance in June 1917 with ‘delusional insanity’. He claimed people were ‘accusing him of being a spy’, that ‘everyone was against him’, and ‘everyone was talking about him’. He ‘threatened to shoot a sergeant’. He stated that his brain was being taken out every night to be experimented on, that his foot was ‘poisoned’, and that he was ‘tortured by Germans during the night’. He disclosed ‘family troubles’. His illness was attributed to ‘stress of campaign’, and he was rated 100% disabled’. He died in Cane Hill Asylum in July 1919.
- Lance-Corporal (TR/6158) Samuel Schoolneart, 14th Battalion King’s Royal Rifle Corps, was discharged on 29 January 1918, aged 30, from the 17th Training Reserve Battalion. ‘Sober and honest’, he had attested in October 1914, when he worked as a labourer. He was in France from November 1915 (Dock Police and APM, having been diagnosed with DAH) until July 1916, when he returned to the UK to be hospitalised in the Lord Derby War Hospital, Warrington suffering from ‘delusional insanity, chronic’, attributable to service, although it was noted: ‘Has not been under fire’. He claimed to have been ‘chased by colonial troops at night, and ‘produced his watch saying “this is my face”’. He died in Cane Hill Asylum 10 months after discharge.
Dementia praecox (schizophrenia)
There were 44 cases of Dementia praecox, 50% of which were deemed aggravated/non-attributable.
- Private (G/3147) Charles William Frederick Fray served in the 29th & 30th(Works) Battalions Middlesex Regiment, and saw home service only. A traveller, he attested in June 1916, and aged 32 was discharged on 14 August 1918 with ‘Dementia praecox’ (there seemingly having been an attempt to discharge him two months after attestation). A medical board on 29 July 1916 recorded the diagnosis of Dementia Praecox which ‘originated some months ago. Not result of & not aggravated by military service. Permanent’. (In July 1917 this was changed to ‘aggravated’).He was admitted to the Cane Hill Asylum on 15 August 1916.Here it was recorded: ‘He began to imagine some months ago that people in the street gesticulated at him and made disparaging remarks about him. Subsequently he imagined that the men at his regiment poisoned his food. Since admission … he has heard voices telling him that he is to be made away with because he is a spy’. It was noted: ‘Of German parentage, hence the nature of the delusions’. He died on 12 November 1918 in the asylum.
- Private (282377) William John Penney, 2/4th Battalion London Regiment, was 24 when he was discharged on 13 May 1918. His character was described as ‘very good, steady & well conducted’. Attesting in December 1915 he has served on the Western Front from 23 January 1917 to 21 June that year. He was wounded (GSW right leg) on 3 June, and hospitalised in Birmingham, from whence he seems to have discharged himself. ‘His mother states that he arrived home … on July 17 1917 in a very exhausted condition & appeared to recognise none of his people. The following day he became violent & threw cups & plates at his mother.’ He was hospitalised two days later in the 4th London General Hospital ‘depressed, taciturn, takes food badly, wandered about aimlessly’. He deteriorated, and was transferred to the Lord Derby War Hospital. Here he was described as ‘mute & sullen’, and in August ‘was violent and persistently knocked his head on the floor’. By November he was ‘restless, incoherent and very unstable’. In February 1918 it was recorded: ‘Memory impaired … obviously confused … admits auditory hallucinations, hears voices that he cannot understand. Depressed and worried. Irritable, and at times becomes impulsive and strikes his fellow patients’. He was diagnosed with ‘Dementia praecox’ – ‘epileptic and insane heredity. Exciting causes: Military service, stress of campaign, GSW of right leg’. He required ‘asylum, constant attendance’. (The comment – ‘hereditary’ – is notable, for in 1910 at the Cardiff Mental Hospital a hereditary condition was identified in 39 per cent of cases.)[145] Penney died in the Cane Hill Asylum on 28 November 1918.
In a number of the cases described above, men died in a county asylum. Such veterans were classified as ‘service patients’, enjoying certain special privileges, including the legal status of private patients.
Mania
There were 28 cases of mania in the pension ledger sample, 100% being regarded as aggravated/non-attributable. These are most often described as ‘recurrent mania’.
- Private (1856) Herbert Tracey Vine was discharged from the 13th Battalion London Regiment on 10 August 1914, having attested four days earlier, and been found ‘fit’ for service (he claimed to have previously served in the 7th Middlesex). He then re-enlisted, Private (1545) in the 2nd East Surreys a month later on 9 September, and served overseas. He was discharged on 14 September 1918 from the East Surrey Depot, so clearly he had been removed from overseas service. His diagnosis was ‘manic depressive insanity’, ‘aggravated’ by service, and he was rated 60% disabled on 22 August 1919. This is puzzling as he is also recorded (in the ‘Soldiers’ Effects’ database) as having died ‘insane’ on 14 September 1918 in the Hanwell Asylum (although this is not listed by Civil Registration).His story reflects his illness. He gave his date of birth on attestation as 1880, when in fact he was born in 1866. A bank cashier, he married in 1892, and was divorced in 1906 for adultery, neglect and cruelty. In December/January 1908-9 he was in the Westminster Workhouse for 8 days having been apprehended by the police in the street, described as ‘emotional’. It seems highly likely that cause of his removal from the army after four days in August 1914 was on psychological grounds – how he was accepted once more is a mystery.
Learning disability
Given that ‘defective intelligence’ was viewed as a ‘general condition of rejection’ for service, it is disappointing to find 72 such individuals (described as ‘feebleminded’ of ‘mentally deficient’ in the ledgers) in the PLS, especially as one might think that this would be readily identifiable on examination.
- Private (205049) John Thomas Dowson, London Regiment, was a 33 year-old single man (whose previous trade was ‘attending wagons’) when he was discharged in March 1919. His ‘invaliding disability’ was ‘feeblemindednes’, date of origin being ‘pre-war’ and his condition was described as ‘constitutional – aggravated’. He was viewed as 20% disabled in February 1919, but in the ledgers in January 1920 as 60% then a month later as 100%. In July 1917 it had been noted: ‘This man does not know his letters’; but on discharge it was written of him: ‘He is dull & slow, lethargic, childish, lacks volition & initiative, well conducted, mental & moral attribute of a low standard’. He did not serve overseas, and his problems were sufficient for him to have been hospitalised from June 1918 to March 1919 (first in The Lord Derby War Hospital, Warrington, and then the Notts County War Hospital), discharged ‘fit to return to care of friends’. He had enlisted into the 4th Battalion Durham Light Infantry (40451) and then transferred to the Army Service Corps and finally the London Regiment. He died of Pulmonary TB in June 1920. It might be thought that Dowson was poorly served as his obviously severe limitations were either missed on entering the Army (or he was accepted on the basis of unskilled employment), and his TB must have been present on discharge.
It might be understandable for John Dowson’s problems to have been ‘aggravated’ by the pressures of the regimental environment, but it is difficult to grasp the attribution of ‘feeblemindedness’ ‘due to’ service (30% disabled) in the case of Private (26942) Henry Ellis, King’s Own Scottish Borderers a 37 year-old single man, who probably did not served overseas, his pension ledger giving no suggestion his disability was acquired.
A number of men falling within this category do not have medal cards which indicates they did not serve overseas. It is possible that their disability was recognised and that this was the cause. An exception is …
- Private (122256) Joseph Adams, RAMC, who was discharged on 5 October 1919, a married man aged 41, with a diagnosis of ‘mentally deficient’ and ‘neurasthenia’ (attributability not stated). He was rated as 20% disabled in September 1920, 40% in 1921, and 30% in August 1922. A ‘presser’ in civilian life, he attested in December 1915, and was mobilized in July 1917. At this time he was ‘porter to No. 9 Coy, Colchester’. His limitations were likely what kept him in the Reserve, and in this particular job. He was sent to Egypt in July 1917, as an orderly in Alexandria, and remained in Egypt. What circumstances led to his neurasthenia are unknown, but it arose in a man with limited coping skills.
Another case illustrates the acceptance of learning disabled man into the pre-war Army:
- Private (28974) Thomas Wellington Bayley, RASC, attested in 1910, at which point he was noted as nearly 19. His pension ledger states that he was born in 1894. His education at this point was deemed ‘third class’, but in 1911 he passed a course in ‘field baking as 2nd hand’, serving as a cook. A Reservist, he went to France on 11 August 1914, and finished his war with 6th Divisional MT Company, although he appears to have continued as a baker until June 1916. He was discharged in March 1919 ‘surplus to military requirements’, but pensioned with ‘mental deficiency’, ‘aggravated’ by service, and 50% disabled. On his pension ledger, ‘aggravated’ is crossed out with ‘att’ substituted, and he was rated 100% disabled, now in an asylum, and he died in June 1920, cause unknown. It raises the question as to whether some other organic process was afoot.
The cases here suggest that rather than necessarily always being missed, the attestation process and medical examinations may have passed men with such developmental problems and retained them on the basis that there were menial jobs for them to do.
Psychological conditions – overview
The estimate of 9% of casualties being psychiatric in nature, and the concordance of this figure with pensions awarded for psychological conditions points towards a low ‘psychological’ casualty rate. This of course is coloured by cultural attitudes to illness.
From the positive point of view, as argued earlier, however certain societal attitudes amongst men may have been protective early in the 20thcentury, primarily stoicism and manliness.From the negative point of view, the discussion above suggests that range of somatic conditions were underlain by psychological factors which were not acknowledged. Diagnostic practices amongst medical practitioners may also have distorted the picture. Certainly, doctors became more willing to acknowledge psychological conditions as the war progressed, and the very fact that men claimed on this basis indicates that there was no personal bar in claimants against doing so, an observation reinforced by the study of the health of postal workers referred to above.
How many men would not acknowledge psychological conditions cannot be reckoned. In a review of veteran unemployment it is noted: ‘The general restlessness of the returned soldiers and sailors made it difficult for many of them to settle down to the humdrum life of their former jobs’.[146] This restlessness may well have been due to raised cortisol levels as a result of the stress of service. The notable irritability of veterans likely had a similar cause. This, there would have been a population of such men with sub-clinical symptoms.
The pattern changed in Second World War. In many respects diagnoses for somatic conditions decreased e.g. effort syndrome/DAH was displaced (even if dyspepsia increased). The increasingly varied definition of psychological conditions were part of this, but also the increased willingness of servicemen to attribute their symptoms to stress, although Jones and Wessely caution that ‘it is by no means clear that psychiatric explanations are significantly more acceptable than they were in the past’.[147] In WW2, 10-15% psychiatric casualties were experienced during the Battle of France (1940); 10-20% in the first two months of the 1942 Middle East campaign; with 11% in the first two months of the Italian campaign.[148] The Ministry of Pensions estimated in 1953 suggest 10% of pensions in WW2 were awarded for psychological and neurological disorders.[149] This is strikingly similar to the picture of WW1.
Final words
This study has focussed on impairment in First World War veterans – its source material could never create understanding of disability as understood by modern disability studies. Nor could dry lists of conditions give insight into the actual experience of disability.
The number of Army servicemen wounded during the war totalled 2,272,998 (this figure counting those who were wounded more than once as a subsequent case), 64% of whom returned to duty, and 18% who returned to non-teeth services. Eight percent were discharged as invalids.[150]
Of the 120,000 pensioners who had died during the post-war decade, ‘only 60-70 per cent were associated with the effects of war service’.[151]This total should, however, rightly be added to the total number of British service deaths during the war.[152]
Mitchell and Smith in the Official History (statistics) concluded that ten years after the war ‘the total cases of serious disablement still remaining’ comprised ‘to the extent of 81.5 percent’ five main disabilities ‘namely wounds, tuberculosis, respiratory diseases, organic diseases of the heart and psychoses’, wounds comprising more than half. At this point, a little over a quarter of servicemen were rated as 30% disabled. This might be seen as indicating substantial adjustment and recovery. Undoubtedly, however, the real human cost of disability remained hidden.
Of the four main medical conditions prominent in pensioners in 1929, approximately 40% of tuberculosis cases, 37% of respiratory conditions, 49% of organic diseases of the heart, and 52% of psychoses were deemed either non-attributable or aggravated by service. This clearly gives a negative picture the state of the health of the nation in an era when medical treatment (largely in the form of effective medications) was in an early state of evolution.
Dr Peter Hodgkinson
Below is a downloadable version of the paper:
Download PDF
Acknowledgements
This project could not have been completed without the assistance of the twenty four volunteers mentioned at the start of this paper. The author and The Western Front Association are very grateful for the hard work undertaken to 'mine' the data used here.
[1] K. Bohta et al. Disability in Industrial Britain, (Manchester: Manchester University Press, 2020), pp.5-6.
[2] http://www.theage.com.au/comment/why-the-numbers-of-our-wwi-dead-are-wrong-20140428-zr0v5.html. See also D.C. Noonan, Those We Forget – Recounting Australian Casualties of the First World War, (Carlton, Melbourne University Press, 2014).
[3] N. Wilson et. al., ‘Mortality of First World War Military Personnel: Comparison of Two Military Cohorts’, British Medical Journal, p.7168.
[4] J. Bourke, Dismembering the Male, (London: Reaktion, 1996), pp.33-37.
[5] Board of Education, Annual Report of the Chief Medical Officer of the Board of Education, 1919 pp.102-3, cited in Bourke, op. cit. p.35.
[6] http://www.swansea.ac.uk/media-centre/latest-news/disabilityinthesouthwalescoalfieldexhibitionrevealsanextraordinaryhiddenhistory.php.
[7] Bohta et al, op.cit. p.143.
[8] Bohta et al, op.cit. p.146.
[9] Bohta et al, op.cit. p.169.
[10] https://www.westernfrontassociation.com/world-war-i-articles/an-overview-of-the-pension-system-immediately-after-the-war/
[11] Yorkshire also exists as a region and surviving records, but its records were not completed in the same way as other regions, with disabilities not specified. Only 2% of the London/South-East records were retained.
[12] T. J. Mitchell & G. M. Smith, History of the Great War Based on Official Documents: Medical Services – Casualties and Medical Statistics, (HMSO, 1931) p.311. This sort of percentage assessment is still used in medico-legal practice and is notoriously difficult.
[13] House of Commons debate on average weekly wages 30/07/1925 (Hansard,Vol 187 cc651-3W).
[14] Cited in Bourke, op.cit. p.61.
[15] Bourke, op. cit. pp.81-4.
[16] J. Collie, ‘The Effects of Recent Legislation upon Sickness and Accident Claims’, Practitioner, (1916).
[17] J. Collie, Malingering and Feigned Sickness, (London: 1917).
[18] https://www.historyandpolicy.org/policy-papers/papers/adapting-the-machine-welfare-policy-after-world-war-one-and-covid-19
[19] Noonan, op. cit.
[20] Although only four spaces were provided on the forms, sometimes five ‘disabilities’ were entered.
[21] Mitchell & Smith, op. cit.
[22] Mitchell & Smith, op. cit. p.275.
[23] Mitchell & Smith, op. cit. p.275.
[24] Mitchell & Smith, op. cit. p.277 (Table 5).
[25] Mitchell & Smith, op. cit. p.317, (Table 4).
[26] Mitchell & Smith, op. cit. p.319 (Table 5)..
[27] Mitchell & Smith, op. cit. p.323 (Table 8).
[28] Mitchell & Smith, op. cit. p.276,(Table 2).
[29]Mitchell & Smith, op. cit. p.279.
[30] Mitchell & Smith, op. cit. pp.335-349.
[31] A Bamji, Faces From The Front, (Solihull: Helion, 2017), p.177.
[32] Bourke, op. cit. pp.45-6.
[33] J. Meyer, Men of War, (Basingstoke: Palgrave Macmillan, 2009) p.98.
[34] PIN 26/19930 J. L. Campbell-White & PIN 26/21230 E. C. Booker, cited in Meyer op. cit. p.106.
[35] PIN 26 /19884 B. Harrison, cited in Meyer op. cit. p.108.
[36] Meyer, op. cit. p.102.
[37] S.R. Graubard, ‘Military Demobilization in Great Britain Following the First World War’, Journal of Modern History, (19) 1947, pp.297-311
[38] J. Winter, & J. L. Robert, Capital Cities at War Vol. 1, (Cambridge: Cambridge University Press, 1997), p.208.
[39] S.R. Ward (ed.), The War Generation, (New York: Port Washington, 1975), p.22
[40] E. Butchart, ‘Unemployment and Non-Employment in Inter-War Britain’, University of Oxford Discussion Papers in Economic and Social History, (1997).
[41] TNA PIN15/722, cited in N. Barr, The Lion and the Poppy: British Veterans, Politics and Society 1929-1939, (Westport: Praeger, 2005), p.81
[42] Bourke, op. cit. p.73.
[43] Bureau of Labor Statistics, op. cit.
[44] Bourke, op. cit. p.53.
[45] TNA PIN 26/19942 J. J. R. Larkin, cited in Meyer, op. cit.p.107.
[46] TNA PIN 26/21555 P. G.Eckersall, cited in Meyer op. cit. p.108.
[47] The King’s National Roll Scheme (the National Scheme for Disabled Ex-Servicemen) was established in August 1919. A review in 1922 noted that numbers were declining, employers had not renewed their contracts, and an estimated 10,000 disabled ex-servicemen were unemployed.
[48] Through higher levels of inflammatory markers. A. Hughes et. al. ‘Elevated inflammatory biomarkers during unemployment: modification by age and country in the UK’, Journal of Epidemiology and Community Health, (2015), http://jech.bmj.com/content/early/2015/02/19/jech-2014-204404.abstract
[49] I. Popovici & M.T. French, ‘Does Unemployment Lead to Greater Alcohol Consumption?’, Industrial Relations(2013), http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3609661/
[50] S.M. Montgomery et. al. ‘Unemployment pre-dates symptoms of depression and anxiety resulting in medical consultation in young men’, International Journal of Epidemiology (1999), pp.95-100.
[51]M.G Macpherson, W.P Herringham, T. R. Elliott & A. Balfour, Medical Services: Diseases of the War Vol II, (London: HMSO, 1923) p.402.
[52]Macpherson et.al. DiseasesVol II, p.409-10.
[53]Macpherson et.al. DiseasesVol II, p. 458.
[54]Macpherson et. al. DiseasesVol II, p.460.
[55]Macpherson et. al. DiseasesVol II, p.517.
[56]Macpherson et. al. DiseasesVol II, p.518.
[57]Macpherson et. al. DiseasesVol II,Table II p.518.
[58]Macpherson et.al. Diseases Vol II, p.519.
[59] Mitchell & Smith, op. cit. p.287-8.
[60]‘Disability and Industrial Society: A Comparative Cultural History of British Coalfields, 1780-1948: Statistical Compendium.’(See Bohta et al. op. cit.)
[61] https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/articles/howhaslifeexpectancychangedovertime/2015-09-09
[62] D. H. L. Brown,D. R. Green, K. McIlvenna, & N. Shelton, ‘The Beating Heart of the System: The Health of Postal Workers in Victorian London’,Journal of Historical Geography, 68 (2020) pp.75-85.
[63] W. Hatchett et al, The Stuff of Life – Public Health in Edwardian Britain, (CIEH, 2012), p.18.
[64] J. C. Riley, ‘The Risk of Being Sick’, Population and Development Review, 16 (1990), pp. 403-432.
[65] R.Floud, K. W. Wachter and A. Gregory, ‘The Physical State of the British Working Class 187-1914: Evidence from Army Recruits’, (National Bureau of Economic Research, Working Paper 161, 1985), p.20.
[66] E. M. Spiers, The Late Victorian Army, (Manchester: Manchester University Press, 1992), p.124-5.
[67] Hatchett op. cit. p.18.
[68] N. Clarke, J. Cranfield & K. Inwood, ‘Fighting Fit? Diet, Disease, and Disability in the Canadian Expeditionary Force,1914-18’, War & Society, (2014), pp.80-97.
[69] Brown,et. al. op. cit..
[70] War Office Instructions issued with Army Orders 1 August 1914, https://www.longlongtrail.co.uk/soldiers/a-soldiers-life-1914-1918/enlisting-into-the-army/instructions-for-the-physical-examination-of-recruits/
[71] J. F. Tucker, Johnny Get Your Gun, (Barnsley: Pen & Sword, 2015), p.13.
[72]I. R. Bet-El, Conscripts, (Stroud: History Press, 2009), p.34.
[73] H.Gleave, letter 12/02/1916 IWM 78/31/ I T.
[74] W. G. Macpherson, Medical Services – General History Vol 1, (London: HMSO, 1921), pp.118-20.
[75] J. F. Thompson, undated letter IWM 72/119/1.
[76] E. Jones & S.Wessely, ‘War Syndromes: the impact of culture on medically unexplained symptoms’, Medical History, 49 (2005), pp.55-78.
[77] The debility cluster was marked by fatigue, difficulty completing tasks, shortness of breath and weakness, with rapid heartbeat, tremor, headache, dizziness, pains in joints, difficulty sleeping, changes in weight and anxiety were ‘moderately represented’.
[78] The somatic cluster was typified by rapid heartbeat, shortness of breath, fatigue and dizziness. Difficulty completing tasks, headache, tremor and anxiety were ‘moderately represented’.
[79] The neuropsychiatric cluster contained a range of bodily symptoms (shortness of breath, tremor, pains in joints, back pain, excessive sweating and the rapid or irregular heartbeat), more notably fatigue, headache, depression, anxiety and difficulty in sleeping. Difficulty completing tasks, forgetfulness, dizziness, weakness, irritability, poor concentration, jumping this, changes in personality, nightmares and weight change were ‘moderately represented’.
[80] Macpherson et. al. DiseasesVol 1 p.227.
[81] Macpherson et. al. DiseasesVol 1, p.231.
[82] B. J. Brabin, ‘Malaria’s contribution to World War One – the unexpected adversary’, Malaria Journal, (2014).
[83]Macpherson et. al. Diseases Vol 1, p.212.
[84] E. Jones, I. Palmer & S.Wessely, ‘War pensions (1900-1945)’, British Journal of Psychiatry, (2002) pp.374-379.
[85] Jones & Wessely, ‘War Syndromes’.
[86] S.Dyde, ‘The Chief Seat of the Mischief: Soldier’s Heart in the First World War’, J Hist Med & Allied Sciences (2011), pp.216-248.
[87] T. Culpin, ‘Disordered Action of the Heart’, British Medical Journal, (1919), pp.394-5.
[88] B. S. Oppenheimer & M. A. Rothschild, ‘The Psychoneurotic Factor in the “Irritable Heart” of Soldiers’, British Medical Journal, (1918), pp. 29-31.
[89] J. A. Venning, ‘The Etiology of Disordered Action of the Heart’, British Medical Journal, (1919), pp.337-9.
[90] P. Wood, ‘Da Costa’s syndrome (or effort syndrome)’, British Medical Journal, (1941), pp.767–72.
[91] M. Jones and V.Mellersh, ‘A comparison of the exercise response in anxiety states and normal controls’, Psychosomatic Medicine, (1946), p.180.
[92] Jones, et. Al. ‘War pensions (1900-1945)’.
[93] Wood, P, ‘Aetiology of Da Costa’s syndrome’, British Medical Journal, (1941), pp. 845–51.
[94] E. F. Bland & T. Duckett Jones, ‘Rheumatic Fever and Rheumatic Heart Disease’, Circulation, (1951) p.836.
[95] Jones et. Al. ‘War pensions (1900-1945)’.
[96] R. T. Grant, ‘After histories for ten years of a thousand men suffering from heart disease’ Heart, (1933) p.275.
[97] Jones et. al. ‘War pensions (1900-1945)’.
[98] Jones et. al. ‘War pensions (1900-1945)’.
[99] Jones & Wessely (2005) op. cit.
[100] Mitchell & Smith, op. cit.. p.70.
[101] Mitchell & Smith, op. cit.. p.69.
[102] Mitchell & Smith, op. cit.. p.71.
[103]Mitchell & Smith, op. cit. p.324.
[104] Mitchell & Smith, op. cit. p.326.
[105] Jones et. al. ‘War pensions (1900-1945)’.
[106] Jones, et. al. ‘War pensions (1900-1945)’.
[107] TNA WO95 344/8, War Diary 36 Casualty Clearing Station (Second Army).
[108] Macpherson et. al. Diseases Vol 1, pp.485-503.
[109] Macpherson et. al. Diseases Vol 1, pp.485-503.
[110] Macpherson et. al.Diseases Vol 1, p.359.
[111] Macpherson et. al.Diseases Vol 1, p.368.
[112] Macpherson et. al. Diseases Vol 1, p.367.
[113] Macpherson et. al.Diseases Vol 1, p.370.
[114] Macpherson et. al.DiseasesVol 1, p.369.
[115]Macpherson et. al.DiseasesVol 1, p.359.
[116] Macpherson et. al.DiseasesVol 1, p. 64.
[117] W. H. A. Groom, Poor Bloody Infantry, (New Malden: Picardy, 1983), pp.33-4.
[118] A. Watson, Enduring the Great War,(Cambridge: Cambridge University Press, 2008) p.248.
[119] MacPherson et. al. DiseasesVol II, p.9. The number of pensions awarded for shell shock and neurasthenia peaked in 1921 at 65,000. (W. Johnson & R.G. Rows, ‘Neurasthenia and the War Neuroses’, in MacPherson, op. cit. pp.7 & 56).
[120] P. Leese, Shell Shock, (Basingstoke: Palgrave Macmillan, 2002).p.10.
[121] The War Office retrospectively estimated that between 5 and 30 per cent of all sick and wounded during the Second World War were psychiatric casualties, this figure largely depending on the type of warfare fought. (E. Jones & S. Wessely, ‘Psychiatric Battle Casualties’, British Journal of Psychiatry, p.243).
[122] J. Winter, ‘Shell Shock’, in J. Winter (ed.), The Cambridge History of the First World War, Volume 3, (Cambridge: Cambridge University Press, 2016), p.332.
[123] P. Hodgkinson, Glum Heroes, (Solihull: Helion, 2016), p.246. Based on the OH’s figure that 2,272,998 servicemen were wounded.
[124] S. Grogan, Shell Shocked Britain, (Barnsley: Pen & Sword, 2014) Kindle edition location 110.
[125] E. Jones et. al., ‘Flashbacks and Post-Traumatic Stress Disorder: The Genesis of a 20th-Century Diagnosis’, British Journal of Psychiatry, p. 160. They are rarely referred to in personal accounts, either. (P.E. Hodgkinson, ‘Human Remains on the Great War Battlefields’).
[126] Report of the War Office Committee of Enquiry into ‘Shell-Shock’, (London: Imperial War Museum, 2004 – first published 1922), p.53.
[127] E. Shorter, ‘Paralysis – The Rise and Fall of a Hysterical Symptom’, Journal of Social History, p.549.
[128] MacPherson et.al. Diseases Vol 2, op. cit. p.2.
[129] T.W. Salmon, The Care and Treatment of Mental Diseases and War Neuroses (‘Shell Shock’) in the British Army, (War Work Committee, 1917), p.36.
[130] C.S. Myers, Shell Shock in France 1914-18, (Cambridge: Cambridge University Press, 1940).
[131] G. Holmes, cited in Jones & Wessely, ‘Psychiatric Battle Casualties’, p.243.
[132]Report of the War Office Committee of Enquiry into ‘Shell-Shock’, p.39.
[133] Jones & Wessely, ‘Psychiatric Battle Casualties’, p.247.
[134] Jones & Wessely, ‘Psychiatric Battle Casualties’, p.247. Once having had such a reaction, a soldier was more vulnerable to a second episode. Of a series admitted to hospital during the months of November and December 1917 just over 20 per cent had previously been hospitalised for shell shock/neurasthenia (MacPherson, op. cit. p.5); and in a study of psychiatric hospital admissions in the Salonika theatre, between 42 and 59 per cent similarly had a previous history of shell shock (Macpherson, op. cit. p.5).
[135] Macpherson et.al. Diseases Vol II, p.5.
[136] P. Barham, Forgotten Lunatics of the Great War, (London: Yale University Press, 2004).
[137] Jones, et al. ‘War pensions (1900-1945)’.
[138] Jones & Wessely, ‘Psychiatric Battle Casualties’.
[139] Report of the War Office Committee of Inquiry into ‘shell-shock’, (London: HMSO, 1922).
[140] Mitchell & Smith, op. cit. p.341.
[141] S. P. Singh and A. S. Lee, ‘Conversion disorders in Nottingham: alive, but not kicking’, Journal of Psychosomatic Research, (1997), pp.425–30.
[142] Asylum Reports, The Lancet, (25 November 1911).
[143] Asylum Reports, The Lancet, (25 November 1911).
[144] Jones et. al. ‘War pensions (1900-1945)’.
[145] Asylum Reports, The Lancet, (25 November 1911).
[146] Bureau of Labor Statistics, U.S. Department of Labor, ‘Public Attitude Toward Ex-Servicemen after World War I’, Monthly Labor Review, (56) 1943, pp.1060-1073
[147]Jones & Wessely, ‘Psychiatric Battle Casualties’.
[148] B. A. Shepherd, A War of Nerves, (London: J Cape, 2000)
[149] Ministry of Pensions, Twenty-eighth Report, (London: HMSO, 1953)
[150] Statistics from the Official History of the Medical Services, summarised at https://www.longlongtrail.co.uk/army/some-british-army-statistics-of-the-great-war/
[151] Mitchell & Smith, op. cit. p.348.This is approximately 2% of those whose who served, whereas the figure given by Noonan in relation to Australian veterans was 3% – it might well be surmised that the British OH figure may be an underestimate for various reasons, including the fact that it deals only with pension claimants and does not include those who received a gratuity/temporary allowance which had expired at the time of death.
[152]702,410 to 31 December 1920 (Statistics of the Military Effort of the British Empire). The total number of British and Empire dead of the war remains unsettled, however.